Left-atrial appendage (LAA) occlusions may help increase cath lab procedure volume.
Interventional thought leaders at the American College of Cardiology (ACC) 2014 meeting shared their predictions about the cutting-edge technologies emerging today that will become commonplace in the cath lab of the future.
“Innovation in medical technology is key to the advancement of medicine,” said Martin Leon, M.D., director, Center for Interventional Vascular Therapy, Columbia University Medical Center/New York-Presbyterian Hospital, New York. He noted mortality from myocardial infarction (MI) has dropped dramatically — by 80 percent since the 1950s — due to technological advancements. He said the next generation of advances will improve operator performance, enable more complex procedures, change the reimbursement system, improve patient and operator safety, and expand the use of minimally invasive cardiovascular procedures into new areas that were previously only the domain of surgeons.
Heart Failure Interventions in the Cath Lab
Leon said several new technologies will soon enable interventional heart failure care. One of the biggest advances in technology, he said, is the CardioMEMS implantable heart failure monitor, which was cleared by the U.S. Food and Drug Administration (FDA) in May. The device is inserted into the pulmonary artery via a transcatheter procedure and accurately monitors pressure to detect fluid retention due to worsening congestive heart failure symptoms. It can detect changes prior to a patient needing hospitalization, when they can be treated with medication, which is hoped to reduce the massive numbers of heart failure readmission rates.
Smaller, fully implantable ventricular assist devices (VADs) will soon be used to help offload the heart to help it heal and put the patient on the road to recovery, rather than the usual downward slope of progressive heart failure. Leon cited the CircuLite micro VAD, about the size of an AA battery, which can be implanted in a minimally invasive procedure via the subclavian artery. It is designed for long-term support of less sick, ambulatory, chronic heart failure patients who are not yet inotrope-dependent.
Another transcatheter technology being developed for heart failure is the intra-arterial shunt device (IASD) by DC Devices. Leon said the permanent heart implant represents a new way to treat diastolic heart failure by relieving blood pressure on the left side of the heart and redistributing it to the right side. It takes about 15 minutes to implant the device and is hoped to help reduce readmission rates and eliminate surgical costs.
New Interventional Therapies Will Include a Menu of Structural Heart Procedures
With declining coronary procedure volumes and many new interventional technologies on the horizon, Leon predicts 50 percent of the financial return from cardiac cath labs will be from non-coronary procedures by 2020. These will include transcatheter valve repairs or replacements (TAVR), left atrial appendage (LAA) occluder placements to eliminate the need for warfarin in atrial fibrillation (AF) patients, peripheral artery disease (PAD) interventions and procedures to correct congenital heart defects.
In regards to coronary stenting, which had been the bread and butter of the coronary cath lab, Leon predicts in the future that 50 percent of patients will receive a bioresorbable stent as the technology begins to replace permanent metallic stents.
Appropriate Use Criteria Will be Needed for Tests and Procedures in the Cath Lab
As healthcare reform continues to move forward and physicians increasingly rely on evidence-based medicine, medical societies are developing appropriate use criteria (AUC) for all tests, procedures and disease states. Leon said in the future, following AUC will become part of reimbursement. In fact, during ACC.14, Congress passed a new Medicare bill that now requires use of clinical decision support for AUC to document justification of expenses charged to Medicare.
In the cath lab, Leon said bread-and-butter stenting procedures may need justification using fractional flow reserve (FFR) data to show a lesion being treated is flow-limiting. He said that for this reason, it will be important that FFR data is captured and recorded in the patient record.
Leon said it is very possible the use of invasive catheter-based FFR in the cath lab might be replaced in the next few years with noninvasive computed tomography FFR (CT-FFR). The CT technology, already in trials, can track the flow of blood through the coronaries to determine FFR pressures for the entire coronary tree. The software also enables virtual stenting to recalculate the flow to see which lesions need to be treated prior to taking a patient to the cath lab.
Advanced Imaging, Guidance, and Planning in the Cath Lab
New imaging techniques will enter standard practice in the cath lab to enable advanced 3-D imaging to facilitate more accurate navigation inside vessels and device placement, Leon said. “This technology is already here and is used today,” he noted.
Most modern angiography systems offer rotational 3-D angiography, which uses a quick spin around the patient to create a CT-like 3-D image of the anatomy, which can all be done tableside in the cath lab. Some systems allow these or CT or MRI (magnetic resonance imaging) 3-D images to be overlaid or fused with the live 2-D fluoroscopic images. This fusion technology is used with TAVR planning and navigation software to better guide precise device placement of procedures, Leon said.
The next step in advanced visualization will be the use of free-floating, 3-D holographic images in the cath lab. Leon said this technology, developed by RealView, is already being used in the prototype stage in a handful of cath labs. It allows physicians to interact with the 3-D datasets, rotating them and even being able to slice through the image on any plane to see cross sections.
Cardiology IT Will Become More Integrated in the Interventional Lab
Information technology in the near future will go far beyond reporting and PACS (picture archiving and communications systems), Leon said. “There is a collision of medical technology and health IT that will produce a unique blend of new technologies,” Leon said.
There is rapid proliferation of tiny and inexpensive patient monitoring devices that will bring new patient monitoring data into patient’s electronic medical records (EMRs). These will be used to better monitor diabetes, heart failure, hypertension and arrhythmias.
Current technology allows 3-D images to be printed by special printers as resin 3-D models. Leon said this technology is now being experimented with, using bio-materials to print custom-made implantable devices, such as heart valves.
Enhanced Intravascular Imaging and FFR Will See Increased Use in the Cath Lab
There have been numerous advances in cath lab imaging system, including technologies on the horizon that may fundamentally change how patients are treated, said Gary Mintz, M.D., Transcatheter Cardiovascular Therapeutics (TCT) co-director and chief medical officer, Cardiovascular Research Foundation (CRF).
While FFR has the ability to identify which lesions are causing ischemia and the modality is recommended to show the need for stenting a patient, FFR requires the use of adenosine. Mintz said a new non-adenosine method called iFR (instantaneous wave-free ratio) was recently validated with a close 90 percent correlation with FFR. He said this will make FFR faster and easier to use, and limit the need for adenosine to only about 30 percent of patients.
Leon said noninvasive CT-FFR from CT scans will likely replace the need for invasive wire-based FFR in the coming years.
The intravascular infrared spectroscopy developed by Infraredx has the ability to identify lipid core plaques based on the chemical makeup of the lesion. It is combined with intravascular ultrasound (IVUS) to show the anatomy of the vessel segment. Mintz said the technology is currently being tested in a trial to pre-emptively identify vulnerable plaques, which are suspected as the primary culprits in acute myocardial infarctions. If the trial proves the technology can accurately identify dangerous, at-risk lesions prior to heart attacks, it may serve as a detection device to preventively treat these lesions to prevent future heart attacks.
Mass General Hospital is developing a combined optical coherence tomography (OCT) near-infrared (NIR) spectroscopy intravascular imaging system. Mintz said this system is similar to the Infraredx technology, but will offer more detail with its high-resolution OCT imaging of the anatomy.
There are pros and cons with both IVUS and OCT, so a hybrid combined OCT/IVUS imaging catheter is in development and has already been used in animal studies, Mintz said. OCT has a resolution of about 10 microns, while IVUS is about 100 microns.
Read the article, "10 Reasons Why You Need Supplemental Imaging in the Cath Lab."
The coming advancement of micro-OCT, now in development, offers resolutions of less than 1-2 microns. Mintz said this would allow easy imaging of individual stent struts and the ability to clearly see tissue coverage.
A recently introduced OCT advancement from St. Jude Medical allows 3-D reconstructions of OCT image datasets. The technology allows a 3-D image of the interor of vessels to be created and presented in a cut-plane view to better identify side branch vessels and to visualize stent malapposition and tissue coverage. Mintz said 3-D OCT might be able to help reduce the need for FFR in many patients because the physician will be able to clearly see issues inside the vessel.
Mintz said there is a high-resolution IVUS system in development that will be downsized into a console that looks like a large iPad device. It will enable fast pullbacks, similar to those used for OCT.
There are already some examples of fusion imaging that co-register CT images with live angiography to improve procedural guidance by showing both the vessel lumen, the radio-opaque markets of the catheters and the surrounding anatomy. Key examples of this are fusion software packages available for TAVR planning and procedural navigation. He said this type of fusion imaging will become much more commonplace in the future and will prove very helpful to steer wires and devices through or around chronic total occlusions (CTOs).
Another type of fusion imaging is co-registered IVUS and angiography. Mintz said this is now offered via the MediGuide system from St. Jude Medical, which displays the position and orientation of devices equipped with a tiny sensor on both live and prerecorded fluoroscopy in real time. Other examples of this type of co-registration for IVUS and angiography were recently released by Volcano and Siemens Healthcare.
Holographic Navigation For Interventional Procedures
Today’s cath lab makes regular use of 3-D technology, including rotation angiography, TEE (transesophageal echo), CT and MRI reconstructions, EP (electrophysiology) lab navigation systems, and structural heart procedure 3-D fusion imaging systems. However, Elchanan Bruckheimer, MBBS, director of the cardiac cath lab, Schneider Children's Medical Center, Israel, said none of these are true 3-D, because they are still viewed on 2-D display screens. “The problem is not the people using the system, it’s the fact that the image data is trapped in the screen,” he explained.
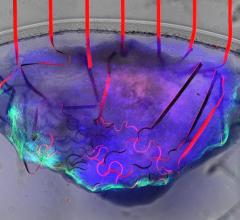
He said this may soon change with the introduction of free-floating holographic imaging, which will allow image projections in the cath lab above the patient where the image can be rotated or sliced through on any axis. He said there has been a prototype system from RealView at his cath lab to display complex cardiac anatomy in holograms. He showed examples of ASD (atrial septal defect) procedures where 3-D TEE holographic images where used for procedural navigation to close the hole using an Amplatzer device. He said the holograms could be rotated to any angle to ensure proper device placement prior to final release of the device and recently completed five procedures using this type of imaging.
He showed examples of how the cardiac anatomy can be segmented using the RealView system, stripping an image of a heart down to the left atrium. He then showed how marks can easily be made on the hologram to show where catheter manipulations are needed for a pulmonary vein isolation. In the future, he said the coordinates of these marks might be transferred into a Hansen robotic EP navigation system to help automate the ablation catheter manipulation to these points.
He said RealView expects to have an operational cart-based holographic system available by 2015.
Robotic PCI
There are now robotic systems available for peripheral, coronary and electrophysiology procedures. Users say these system greatly improve their accuracy in vessel navigation and procedural precision, even among experienced well-known operators.
“Why do we need robotics? We need it to improve procedural success, patient safety and operator safety,” said Giora Weisz, M.D., Shaare Zedek Medical Center, Jeruselum, Israel. He shared his experience using the Corindus CorPath system for percutaneous coronary interventions (PCI).
Despite how experienced an operator may be, they still have limited control of interventional devices within the body. He said this frequently translates into geographic misses with stent coverage which can contribute to adverse events. Geographic misses also contribute to the 13-32 percent of cases where a second stent is needed.
Weisz was involved in the FDA pivotal trial, where there were zero complications and a 99 percent procedural success rate without the need to convert to a manual procedure, which was the trial’s primary endpoint. He said overall the trial data showed the robotic system helped reduce procedural time and increase accuracy when navigating devices inside vessels.
The operator uses joystick controls to navigate vessels on a screen in front of them while seated in a lead-lined cockpit. There is a robotoc catheter drive unit attached to the patient table that utilizes a single-use cassette that enables any off the shelf devices to be used.
“Intravascular manipulation of devices is easy and intuitive using the system,” Weisz said. The FDA approval study only looked at use of the CorPath in straightforward easy PCI cases, but he said in an ongoing post-market study, the system is being used in more complex cases.
During traditional procedures, interventional cardiologists are exposed to radiation and need to wear heavy lead aprons. The excessive weight causes fatigue and about 70 percent reported they now have serious back problems in a Society of Cardiovascular Angiography and Interventions (SCAI) survey. From a dose perspective, Weisz cath lab staff receive an average of about 20.6 mGy of dose per procedure, but with the CorPath system operator’s booth, that level was reduced 95 percent to just 0.98 mGy.
Technologies for Reducing Radiation in the Cath Lab
Leon said ionizing radiation from medical imaging has become a growing concern among the public and medical community, but new technologies can help reduce dose. Cardiac imaging accounts for about one-third of the source of radiation dose from medical imaging. In the cath lab, as transcatheter procedures become more complex and require longer imaging times, radiation exposure to both patients and operators is increasing.
“We are working pretty much the same way in labs today or the as we did more than 30 years ago,” said James Goldstein, M.D., director of research and education, cardiovascular division, William Beaumont Hospital. This means safety has not improved much, as operators still wear heavy lead aprons which cause long-term back and spine issues, and radiation exposure to the eyes causes a high rate of cataracts. He cited studies showing 60 percent of interventional cardiologists have spine issues and 51 percent have the beginnings of cataracts.
“The badges don’t protect us, and about 50 percent of interventional cardiologists don’t wear their badges anyways, because they don’t want to get pulled out of the lab,” Goldstein said.
He made the analogy to the NFL ignoring concussion issues for years and knowing concussions had long-term effects on the lives of football players, but doing nothing about it. “We go into the cath lab today dressed like football players in the 1950s with leather helmets and no faceguards or other protection,” he said.
However, he said new technology is available to address radiation and taking the cath lab staff and the operator out of the radiation field by using robotic systems from Stereotaxis, Hansen and Corindus. There are also new radiation protection systems available to help block radiation scatter. These include the RadPad and Trinity radiation protection systems, and the ZeroGravity ceiling gantry mounted lead suit system that takes the weight of lead aprons off of physicians.
Newer, large format displays now available for cath labs enable a larger field of view and better visualization of the anatomy, instead of leaning over the table to try to see anatomic details on smaller screens, said John Messenger, M.D., FACC, director, cath labs, University of Colorado. This helps better visualize procedures and helps lower dose by not needing to image the anatomy several times.
He said all the major vendors recently released newer angiography systems with dose lowering technologies, including new X-ray tubes, and more sensitive detectors and software to help improve image quality at lower doses, including noise reduction. He pointed to the Philips Allura Clarity as an example of the next-generation angiography system, which can lower standard procedural dose by 50 to 75 percent. He said the operator can easily adjust the frame rates to help reduce dose.
The University of Colorado is using a new Allura Clarity system, and when comparing it to older Philips Xper systems, they found an average reduction of 750 mGy with a more than 50 percent reduction in dose. “These are very striking reductions in dose,” Messenger said.
Messenger said Toshiba’s Spot Fluoroscopy software for its Infinix-i systems allows clinicians to observe a target region of anatomy using Spot Fluoro’s live fluoroscopy, while viewing the last image hold (LIH) in the surrounding area that has been collimated out of the field of view to cut dose.
He said the Mayo Clinic began a program to lower its radiation dose through best practices. It began use of the dual-axis rotational coronary angiography (DARCA) technique, which uses a rotation of the gantry around the patient with simultaneous left to right and craniocaudal movements. This allows complete imaging of the left or right coronary tree with a single acquisition run. The technique helped lower both contrast and imaging dose, and helped achieve a 50 percent dose reduction in radial access procedures.
MRI Could Replace Angiography
Ionizing radiation could be completely eliminated from the cath lab if the angiography system is replaced by MRI image guidance. The cath lab at the National Institutes of Health (NIH) has one lab that uses MRI instead of X-ray angiography to visualize procedures inside patients. The advantage of MRI is that it can visualize all the patient’s anatomy, not just an X-ray of unblocked coronary artery lumens. Another advantage is that MRI does not use radiation to image, so it is safe for patients during longer procedures and the physician can use live imaging during the entire procedure. Additionally, cath lab staff and operators do not need to wear lead.
“We don’t have to wear lead, but we do have to wear headsets to be able to speak to each other over the annoying noise of the MRI system,” explained Robert Lederman, M.D., from the NIH cath lab. “All you need for this is an experienced cardiovascular MRI tech to help with the imaging.”
MRI shows all of the soft tissue anatomy in the field of view, including chambers of the heart and blood flow, which can help visualize clots or pulmonary embolisms. “One of the great things about MRI is that you can see where your catheters are going,” he said.
NIH has designed a guidewire with a tip that serves as an MRI receiver. The tip lights up in bright fluorescent green on the MRI to clearly see where it is in the anatomy. Lederman said this has been very helpful for procedures such as transseptal punctures. “Under MRI the procedures are very relaxed and controlled, because you can see what you are doing and what tissue your needle is going through,” he explained.
Transcatheter closure of PFOs and other holes in the cardiac septum is usually assisted under angiography with TEE. Under MRI, Lederman said adjunct imaging is not needed, because the operator can clearly see the hole, the septum, chambers and the device all at once.
The NIH worked with Children's National Medical Center in Washington, D.C., to create the first pediatric MRI cath lab in the country, which is opening in 2014.
Related articles on future technologies in cardiology and healthcare:
Cardiovascular Advances to Watch in the Next Decade
The Future of 3-D Printing in Medicine
VIDEO: Editor's Choice of Future Healthcare Technologies at HIMSS 2015
 April 12, 2024
April 12, 2024