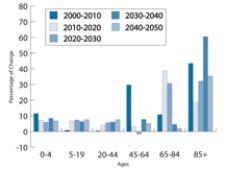
Figure 1 - As the demand for cardiology services is increasing, the supply has not kept pace.
In 2006, the baby boom generation (those born from 1946 - 1964) started turning 60 at the rate of 330 per hour, according to the U.S. Census Bureau. By 2031, almost 60 million baby boomers will be over 65. See Figure 1.
Looking at the coming tsunami of seniors raises a lot of issues, especially in cardiology. Along with reaching their golden years, this generation will also be entering the peak cardiovascular disease years.
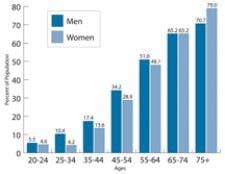
The trailing edge of the boomers is turning 43 this year while the leading edge is turning 61. According to the statistics collected by the CDC/NCHS (Figure 2), this means the prevalence of cardiovascular disease moves from an average of 15.5 percent of the population for the younger boomers to an average of 50 percent of the older population with CV disease. By 2031, the incidence of CV disease will be 65 to 75 percent of this population or 40 to 45 million new potential patients.
Cardiovascular disease remains the No. 1 cause of death in the U.S. Almost twice as many Americans die from cardiovascular disease than from cancer, the nation’s second leading cause of death. (CDC/NCHS 2001). The AHA publication, “Heart Disease and Stroke Statistics - 2004 Update” states that nearly 2,600 Americans die of CVD each day, an average of one death every 34 seconds.
“CVD claims more lives each year than the next five leading causes of death combined, which are cancer, chronic lower respiratory diseases, accidents, diabetes mellitus, and influenza and pneumonia,” the report continues.
Unfortunately, as the demand for cardiology services is increasing, the supply has not kept pace. As documented by Drs. Kereiakes and Willerson, among others, the current and ongoing shortage of trained cardiovascular specialists is due, in part, to a program in the mid 1990s that focused on limiting the cost of cardiac care by reducing the number of cardiology training programs and trainees.
The effect of reducing the number of cardiology fellowships remains with us today. Craig Walker, M.D., The Cardiovascular Institute of the South, reports that his group and “every key group in America is looking for additional cardiologists and is not able to find them.” The dwindling number of U.S. trained medical students entering cardiology programs had been somewhat offset by an increasing number of international school medical graduates. However, the change in immigration policies has now limited that source as well.
Increasing the number of cardiologists and short-tracking the training program are options still under discussion — five years after the ACC Task Force on Work Force was initiated. One of the working groups of the ACC Task Force on Work Force was using technology to increase efficiency and productivity.
Can technology be employed to improve cardiologist productivity and help manage the enormous, oncoming wave of cardiovascular patients? All too often, it seems that new technologies manage to increase the burden of the practitioner.
But given the magnitude of the problem, increased productivity should be a primary requirement of new systems.
Access Anywhere
Many institutions have invested in a variety of cardiovascular information systems that will ultimately allow the cardiologist to work anywhere, providing access to diagnostic information and reporting tools. Network systems currently eliminate the time lost now by having cardiologists travel to where the information is stored, for example, in the cath lab or on a speciality workstation. One of the best examples of how technology can improve productivity is in the echocardiography laboratory.
For those echocardiographers who have made the switch to digital echo and reporting, there can be an associated bonus of decreased workload. Several labs have reported that reading and reporting time decreases substantially, usually by 30 percent. Gregory A. Rose, M.D., director, Cardiac Ultrasound Laboratory Sanger Clinic/Carolinas Medical Center Charlotte, NC, reports the experience of three busy labs in a white paper on ASE's (American Society of Echocardiography) Digital Zone.
After reviewing the reading and reporting processes in a digital lab, Dr. Rose found that “physician review time is decreased by five minutes per study: this translated to 25 full work days that are ‘given back’ to the physician,” assuming 2,500 studies per year. Digital labs have found productivity improvements for sonographers as well since they spend much less time performing administrative chores. As the volumes increased by 100 percent, the corresponding increase in staff was 50 percent.
Patty Johnson, system director, Cardiovascular Services at Lee Memorial Health System, remains amazed at the difference digital echo has made for their cardiologists. Lee Memorial Health System was a three-hospital system with two major outpatient clinics when digital echo was fully deployed with the addition of structured reporting. Two more hospitals were added early this year making Lee Memorial Health System a five-hospital system.
Although one of the hospitals was the primary cardiology center, cardiologists still had to staff all the hospitals and outpatient centers to read echocardiographic studies. On a good day, it takes 30 minutes to travel between any two of the hospitals. Now, with the deployment of digital echo across the system and a robust WAN, cardiologists can read wherever they are working. Johnson reports they now read echos wherever they are working, even between cases in the cath lab. Cardiologists no longer have to make a trip just to read as they did with VCR tapes. Even now, according to Johnson, the cardiologists are still saying that “this is the best thing that the hospital ever did for us.”
Not only is the travel time eliminated, but the reading and reporting time is reduced as well. Instead of “wading through all that tape,” the cardiologist can use the thumbnails to go right to the images that are germane. A normal echo study can be read and signed with just two clicks. Plus, access to priors is instant — no matter how old the study is. Older exams used to have VCR tapes stored in two off-site locations and could take as long as two days to retrieve.
Unfortunately, the digital experience in the cardiac catheterization laboratory has not been as encouraging to date. Access to prior exams is dramatically improved over the days when cardiologists waited while radiographic technologists prowled the basement hunting down a prior exam. However, the practice of a cardiologist reading a report printed from a hemodynamic system into a transcription system is all too common.
CT Boosts Efficiency
Another technology that has been touted as increasing physician efficiency is Cardiovascular CT. CVCT does not require a physician to perform the exam, and it is much faster than conventional angiograms of cardiovascular structure.
CVCT has been enthusiastically adopted by the physicians at The Cardiovascular Institute of the South. The group’s use of CT has grown from one 16-slice scanner three-and-a-half years ago to four 64-slice scanners today at four of its primary locations.
At this time, instead of diagnosing coronary disease, these scanners are employed in diagnosing peripheral disease. Dr. Walker says it has become the tool of choice for peripheral studies because “it uses less dye, is noninvasive, more accurate and less expensive than a conventional arteriogram.” In addition, he notes that CVCT has ancillary findings that one would not find in a conventional study — for example, a renal stenosis as part of a runoff exam.
And producing better results is not the only benefit. Unlike a conventional angiographic study, which requires 30 to 40 minutes of a physician’s time, a CVCT exam does not require a physician to actually do the exam — only to read it at his convenience.
Today, the cardiologists at The Cardiovascular Institute of the South find that coronaries make up only about 10 percent of the volume on their CT scanners. Given issues primarily with calcium artifacts and difficulty getting quality exams with arrhythmic patients, the group uses the scanner for coronaries on low motion bypass grafts and to screen out false positives from other tests on patients with low calcium scores and low heart rates.
Dr. Walker sees the potential for cardiac CT to become a large part of their practice when CVCT's temporal resolution improves, which should be the case with 256-slice scanners now on the horizon. Along with a safer exam will come improvement in cardiologist efficiency, similar to what the group currently experiences with peripheral CT exams.
However, technology will not substitute for the “one-on-one, doctor-patient relationship where they meet to find what is going on,” noted Dr. Walker. Technology can help improve cardiologist efficiency and that should be a requirement for all new systems, but technology cannot substitute for a well-trained cardiologist.
It should also be noted that, just as in many other fields and industries, a large number of cardiologists are baby boomers themselves.

 February 06, 2026
February 06, 2026 







