Endovascular aneurysm repair (EVAR) using transcatheter-deployed stent grafts has grown significantly in the past 10 years. While surgeons traditionally perform aneurysm repairs, experts say the devices are increasingly deployed in cath labs by interventional cardiologists.
The number of abdominal aortic aneurysm- related deaths have declined since the introduction of EVAR, according to an ongoing, long-term research report from Beth Israel Deaconess Medical Center in Boston. The most recent update was released in the March issue of the Journal of Vascular Surgery.
“We have found that use of EVAR, which was approved by the Food and Drug Administration in 1999, has increased steadily and in 2005 accounted for 56 percent of repairs, yet only 27 percent of the deaths for intact repairs,” said senior study author Marc L. Schermerhorn, assistant professor of surgery, Harvard Medical School and section chief of endovascular surgery at the center's department of vascular surgery.
EVAR is also on the rise according to the University of Massachusetts Memorial Medical Center, Worcester, MA, where the Accreditation Council for Graduate Medical Education database was reviewed to see the volume and type of procedures performed by graduating vascular trainees from 2001 to 2007. EVAR procedures increased by 299 percent, while the volume of open surgical procedures largely remained stable.
The benefits of EVAR include shorter procedure time, eliminating the need to undergo a large abdominal incision and clamping of the aorta (which creates significant stress on the heart), reduced patient trauma, reduced hospital stays and faster recovery. EVAR is performed through two small groin incisions and is often feasible for patients when a traditional surgery cannot be performed due to other morbidities.
“The number of endovascular repairs is going up,” said Michel Makaroun, M.D., professor and chief of the division of vascular surgery, University of Pittsburgh Medical Center, and president of the Association of Chairs in Vascular Surgery, a section of the Society for Vascular Surgery. Today, he says, between 50-60 of aortic aneurysms are repaired endovascularly.
“There is no question that the number of patients being treated endovascularly is going up and the number treated surgically is going down,” said Michael Davidson, M.D., division of cardiac surgery, Brigham and Women’s Hospital, Boston.
He said part of the reason for the increase is the safety record of the devices and comparable outcomes to surgery. Several studies in the past year showed very good outcomes for EVAR.
“Our experience has been, in carefully-selected patients, endograft outcomes are at least as equal to surgical procedures,” Dr. Davidson said.
The first generation of EVAR devices in the mid-1990s had issues with endoleaks (where blood continues to flow into the aneurysm sac), fixation and defects in manufacturing or materials used, Dr. Makaroun explained. Poor fixation caused late migration of the devices. Some fabrics leaked, stent polishing techniques contributed to fatigue strut failure, and there were questions about how much devices should be overlapped.
However, today Mr. Makaroun said EVAR devices achieve a level of reliability on par with surgical repair. “There have been a lot of advancements over the past 10 years,” Dr. Makaroun said. “The results are getting better and better.”
He said in the late-1990s endovascular aortic repairs were usually only stable for about two or three years, but today’s devices offer stability of at least eight or nine years. Better fixation systems have also made migration mostly a thing of the past, Dr. Makaroun said.
Complications associated with EVAR include endoleaks due to a poor seal of the device, or caused by late migration of a stent graft. Dr. Davidson said repairs to seal these leaks include putting in extender cuffs, deploying a second stent graft over the first, or injecting coils or thrombin into the sac.
“If you get into migration, your options are to place a second device or open surgery,” he said.
Transitioning From ORs to Cath Labs
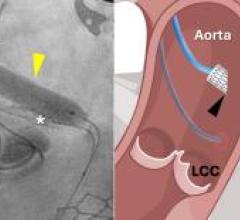
Endovascular grafting of straight sections of the aorta can be done using low-quality mobile C-arms, but more difficult jobs, especially around side branch vessels, requires better images from fixed C-arm systems, as found in cath labs. This has given rise to these procedures being performed more often in hybrid cath lab/ORs.
“There is absolutely no reason why these devices cannot be used in the cath lab,” said Bart E. Muhs, M.D., assistant professor of vascular surgery and radiology, co-director of endovascular surgery, department of surgery and intervention radiology, Yale University School of Medicine in New Haven, CT.
“Right now it’s about 50/50,” Dr. Muhs said of his assessment between surgical and EVAR cases. But, he believes within the next five years, the majority of EVAR cases will be performed percutaneously. Dr. Muhs performs about 90 percent of the EVAR procedures at Yale. Of these cases he said many of them are performed in the cath lab. He said the size of the devices, down to an 8 Fr., allow cath lab usage without the need for surgery.
However, if a complication arises, it is easier and safer to use a hybrid cath lab/OR. “EVAR, that's the poster child for hybrid ORs,” he said.
At the University of Pittsburgh Medical Center, Dr. Makaroun said all endovascular aortic repairs are done in a hybrid OR in case surgical interventions are required. He said hybrids are becoming the standard of care in most institutions that have a large number of these repairs.
Brigham and Women’s uses hybrid cath labs for these procedures and Dr. Davidson said the environment at his facility is very cooperative between the various specialties. He said this cooperation helps when skill sets from vascular and cardiac surgeons and interventional cardiologists are needed in the hybrid environment, leading to better patient outcomes. Hybrid labs performing these procedures will need even more cooperation between specialists as more devices are introduced and techniques require higher levels of expertise, he said.
“The places that are going to be most successful are the ones with the least amount of infighting,” Dr. Davidson said. “As procedures become more complicated you will need additional skill sets from other specialties.”
Dr. Davidson said endovascular repairs are being done by vascular surgeons, interventional cardiologists and interventional radiologists, but the primary providers are still cardiac surgeons.
“The surgeons have had more of a role because of the size of the devices,” Dr. Davidson said.
He said most devices require a 24 Fr. catheter, and in about 15 percent of his cases surgical exposure of the iliac arteries is needed to insert the catheter. He said the surgical prospect makes many interventionalists shy away now, but as the technology improves and devices become smaller, more interventional cardiologists may undertake these repairs.
Dr. Makaroun said the device sizes in the mid-1990s were 25-26 Fr., today devices are around 18-22 Fr. New generations are being developed as small as 14-16 Fr. However, size alone will not determine if more cath labs take on aortic repairs. He feels surgeons are still the best qualified because they offer more options to patients and can switch to surgical techniques in case of complications.
Changes in EVAR Technology
The current technology allows easy stent grafting of straight sections of the aorta. But, it is more difficult to repair and properly seal aneurysms around side branch vessels.
“These patients have been previously excluded where aneurysms are near the side branches,” Dr. Davidson explained. “The straight tube ones are pretty easy, but side branches are very tedious and require more expertise.”
He said the next generation of stent graft devices now being developed by manufacturers will allow grafting of side branch vessels, such as the renals, iliacs and head vessels. New devices are also being created to deal with aortic dissections.
“Technologies are now coming out to address areas where we would not have even attempted endovascular repairs a few years ago,” Dr. Makaroun said. “There is practically no region of the aorta that we will not be able to repair endovascularly... In the next few years the envelope of the technology will be pushed with the availability of these new devices.”
He said vessel tortuosity and repairs around side branch vessels can make these procedures difficult. Stent grafts can also occlude collateral vessels. But, he said the next generation of devices hold promise to overcome these issues.
New devices currently available in Europe, and in some cases working their way through FDA approval, will allow repairs near or on top of side branches. This will allow better, long-term device fixation in the more stable area around the renals, Dr. Makaroun said. He said the region of the aorta below the renals tends to be unstable, resulting in aneurysms. Even if stent grafts are placed on a stable area of the aorta below the renals, the vessel can continue to deteriorate and cause leaks or migration.
Dr. Muhs, who is working with some of Cook Medical’s EVAR devices in FDA trials, has seen the technology progress quickly over the past few years with incremental improvements. He said this evolution will continue with smaller delivery systems, device choices based on anatomy, more customized devices and more flexible devices.
For More Information
www.crbard.com
www.endologix.com
www.goremedical.com
www.jvascsurg.org
www.medtronic.com
www.VascularWeb.org


 February 13, 2026
February 13, 2026