The Corindus CorPath robotic system allows interventional cardiologists to navigate coronary vessels without the need to be in the radiation field.
Hospitals constantly try to predict what the future holds when planning new facilities and equipment purchases that will need to last for the next decade. Martin Leon, M.D., director of the Center for Interventional Vascular Therapy, Columbia University Medical Center / New York-Presbyterian Hospital, attempted to answer that question for interventional cath lab technologies during Transcatheter Cardiovascular Therapeutics (TCT) 2012, making predictions through 2020. Leon is the founder and a director of TCT.
“This is really the greatest period of time in the history of interventional cardiology,” Leon said of the new technologies and trends of today that are shaping tomorrow.
He said the biggest change will be in the types of procedures performed in the cath lab. New types of more complex procedures and devices, recently introduced or currently in trials, will increase cath lab volumes. These include transcatheter aortic valve replacement (TAVR), renal denervation to treat drug-resistant hypertension, transcatheter structural heart repairs such as patent foramen ovale (PFO) and ventricular septal defects (VSDs), and left atrial appendage (LAA) occlusion to eliminate warfarin therapy in atrial fibrillation patients. Some procedures, especially hybrid coronary revascularizations and TAVR, combined with healthcare reforms, also will require new levels of collaboration between various specialists, such as surgeons and the interventionalists.
“It’s a complete transformation from what we are doing in the cath lab today,” Leon said. “We will be serving many users, not just cardiologists.”
New Players and Procedures
The key consideration will be the culture change in the cath lab, which is moving away from only serving the cardiologists to an array of other users. The cath lab of tomorrow needs to consider all these players, which Leon said includes interventional radiology, electrophysiology, peripheral interventions, vascular surgery, interventional neurology, structural heart procedures and interventional oncology.
In many cases, this will involve hybrid procedures, mixing components of both surgical and interventional therapies, giving rise to the hybrid operating room (OR) or hybrid cath lab. These rooms are built to facilitate both surgical and interventional procedures, with proper equipment, ventilation, sterility and high-quality fluoroscopic imaging systems.
“It gives you multidisciplinary capability so we can start working together,” Leon said of these rooms. “We have five hybrid labs at Columbia we now share with the surgeons and it has become the norm.”
In light of lowering healthcare costs, increasing less invasive techniques and new technologies entering the cath lab, Leon said many procedures will become same-day discharge.
“Reimbursement and other factors are going to force us to move toward out-patient procedures,” he explained. “We can’t afford having complications we can’t see because we did not have an echo machine available, as in TAVR. More complex procedures require more complex tools.”
IT Integration
All systems in the cath lab need to be integrated from an information technology (IT) standpoint. Disparate systems should no longer be used. Leon said integrating IT saves staff time and makes the transfer of information much faster and efficient, whether it is patient hemodynamic information, inventory control, imaging, reports or transferring data to registries. He said all the technology used in the cath lab will need to interface with a central cardiovascular information system (CVIS).
Cath labs are replacing old CRT monitors and arrays of first generation flat-panel monitors with a single, large-screen, high-definition, flat LCD monitor. Leon said these large-format monitors can show a single image or be divided into multiple screens to display multiple modality images of the patient. The larger displays also help reduce the need to strain or lean over patients to clearly view the images, Leon said.
Imaging in the cath lab will also require more integration. Instead of stand-alone cart for intravascular ultrasound (IVUS), optical coherence tomography (OCT) or fractional flow reserve (FFR) systems, these will be directly integrated in the cath lab.
Another area of IT integration will be automated inventory management systems. Leon said theses systems will help keep track of medical devices and disposables used during procedures and automatically attach the items for billing.
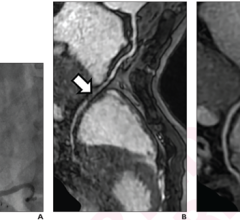
CT-FFR Preprocedural Planning
Although still being validated, Leon said one of the major imaging advancements that will have an impact on the cath lab is computed tomography FFR (CT-FFR). This will allow noninvasive FFR readings for the entire coronary tree with one CT scan. Not only will cardiologists immediately be able to identify culprit lesions with quantifiable, significant flow restriction, but it allows implantation of a virtual stent or stents to see how it impacts flow. Leon explained this tool will enable cardiologists to plan the access route and take extremely accurate measurements so a personalized procedural kit for each patient can be assembled for required guide catheters, wires, balloons and stents. The tool should also greatly speed procedure times, since diagnosis and planning will have occurred ahead of the procedure.
Periprocedural Guidance
The use of 3-D rotational angiography will increase in coming years because it offers the ability to create 3-D image models of the anatomy immediately in the cath lab while the patient is on the table. Leon said these images are extremely good navigation aids because the physician can see all the anatomy, instead of just a 2-D image contrast in unblocked vessel lumens. He believes 3-D imaging will be incorporated on all new angiography systems and will see increasing integration with other imaging modalities and live angiography to greatly enhance transcatheter procedural visualization inside the body.
New generation fluoroscopy systems offer an array of procedural guidance software to merge 3-D images from a variety of modalities with live fluoro, he explained. This will also include immediate registration with ultrasound and transesophageal echo (TEE), both of which are seeing increasing use in the cath lab. Some of the new structural heart transcatheter procedures, especially mitral valve repair, are not possible without 3-D/4-D echo guidance, Leon said.
This level of 3-D integration with live fluoro also will enable more routine interventional treatment of chronic total occlusions (CTOs). “There are so many short-comings with CTO imaging. Clearly if we had better imaging we could more easily treat these lesions,” Leon said. Real-time integration of live 3-D/4-D ultrasound and fluoro will enable much easier guidance.
Robotics
The rapid adoption of Da Vinci surgical robotic system in the OR has helped make procedures less invasive, more accurate and faster. The same is expected of the recently introduced Corindus system for interventional coronary procedures, and the Hansen Magellan peripheral vascular interventional robotic system. Leon said both systems take the interventionalist out of the radiation field and allows them to sit in a chair, without wearing lead aprons, and precisely navigate vessels using video game-style joysticks.
In trial, he said the Corindus system reduced the physician’s radiation dose by 95 percent.
Leon said by 2015 it is estimated there will be more than 1 million robotic procedures performed annually.
Mobile Angiography Systems
Hybrid rooms require a lot of space to accommodate extra surgical and anesthesia equipment and to enable better patient access. For this reason, Leon said there is increasing use of ceiling mount gantries for the angiographic C-arm and much of the other equipment in the room. These gantries allow equipment or the C-arm to be swung out of the way. Leon mentioned the FlexMove gantry system offered by Philips Healthcare as the type of solution that will be common-place in tomorrow’s hybrid rooms.
GE Healthcare’s new Discovery IGS 730 angiography system may show the way of the future, Leon said. It eliminates the need for either a ceiling or floor mount gantry. Instead, it uses a wheeled base and a precision laser guidance system, offering the same high quality imaging and features of a fixed gantry system, but the versatility of a mobile C-arm.
Appropriate Use Criteria
Appropriate use criteria (AUC) is becoming the basis for decision-making today regarding numerous diagnostic tests and therapeutic procedures and will have a major impact on medicine in the next couple years.
“This is going to be one of the influences on the future,” Leon said.
AUC will see increasing integration in the cath lab to guide procedures, especially since future reimbursement may depend on its utilization. Health IT meaningful use criteria also will require the implementation of AUC clinical decision support software, which will likely see integration in cath lab computer systems and cardiovascular information systems (CVIS).
Radiation Protection
The weight of lead aprons limits physician mobility and causes fatigue. Long-term, Leon said this leads to orthopedic issues in most interventional cardiologists. New, lightweight, ultra-thin, disposable radiation protection is now available and will likely become the new normal in cath labs. He said Mayo Clinic is currently using this technology to lighten the load.




 October 24, 2025
October 24, 2025