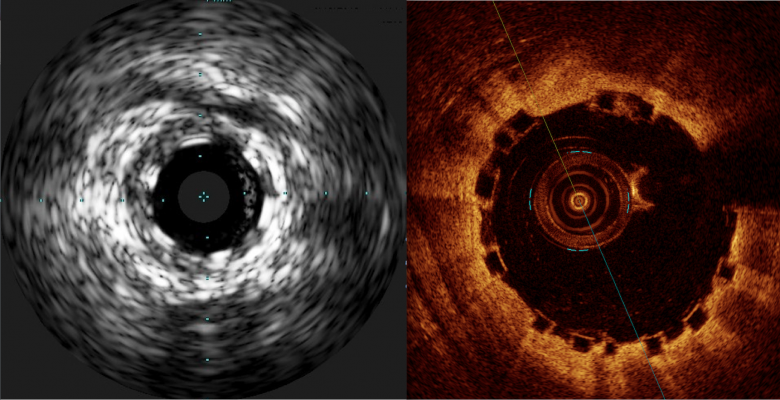
A comparison of how the Abbott Absorb BVS appears with intravascular ultrasound (IVUS) on the left, and optical coherence tomography (OCT) of the right. The stent is difficult to visualize and sizing is critical, so both modalities can help in bioresorbable stent measurements and to confirm stent apposition. Left image from the Volcano IVUS system and the right image from St. Jude Medical's OCT system
There has been a lot of interest in the interventional community regarding the Abbott Absorb Bioresorbable Vascular Scaffold (BVS) since its U.S. Food and Drug Administration (FDA) approval in July. While adoption of this new, first-in-class bioresorbable stent has been embraced enthusiastically by many hospitals, there are important limitations to the device, which dictate how it needs to be deployed, patient selection and, most crucially, the need for very accurate measurements and deployment.
One tool that may help increase the precision of measurements and deployment is the use of robotic catheter navigation systems. The first robotic-assisted case involving the deployment of an Absorb stent took place in September. Paul Campbell, M.D., FSCAI, FACC, cardiologist at Sanger Heart and Vascular Institute, Concord, N.C., Carolinas HealthCare System Northeast, used a Corindus Corpath robotic system to perform the procedure. He said there are several advantages to using robotics for the BVS. The main reason is because of the robot’s enhanced visualization and millimeter-by-millimeter advancement capabilities to address the multiple challenges of this stent.
The First Robotic Bioresorbable Stent Procedure
The case involved a 48-year-old man who had a stable, non-STEMI lesion in his left anterior descending (LAD) artery. Campbell said the lesion was located at the take-off for a side-branch vessel bifurcation. He chose an Absorb stent because of the bifurcation, wanting to preserve future therapy options for the patient and prevent jailing the side branch.
“This is an ideal patient for a BVS due to the bifurcation,” Campbell said. “This is a 48-year-old man, so if he needs to come back in a few years, that stent will be gone.”
He said the lesion was prepped using conventional balloon angioplasty, followed by an exchange to the stent delivery balloon. The stent is delivered on a compliant balloon that is inflated to about 6-10 atmospheres. It is then exchanged for a non-compliant balloon for final expansion of the Absorb. Campbell said the Absorb can be post-dilated by about 0.5 mm, but beyond that may fracture the struts. For this reason, he said it is extremely important to properly size the vessel and use a stent that fits properly.
He used a 3.5 mm Absorb that was post-dilated to 4 mm. He said this helps embed the struts into the plaque and the vessel wall, pushing it out of the way for increased lumen gain. Campbell said this is important with the Absorb, because it has a strut thickness of 156 microns, which is about twice the size of most conventional metallic stents. For comparison, the Xience V is 81 microns, the Endeavor and Resolute stents are 91 microns, and the old workhorse Cypher stent from several years ago was 140 microns. The thickness issue becomes more acute when Absorb stents are overlapped, Campbell said, since it creates 0.6 mm in lumen loss just from the layered struts.
Due to the stent’s inability to be overexpanded, it is not recommended for some lesions. “It does not have the same radial force as a metallic stent, so you cannot use it in calcified lesions,” Campbell said.
He increased the angiography imaging system's frame rate to 15-30 FPS to enable easier visualization of the two sets of radiopaque markers embedded in the ends of the stent since, being made of bioresorbable plastic, the stent is otherwise invisible on fluoroscopy.
“You have a device that is hard to visualize anyway, so you should do anything you can do to improve your visualization of the device,” Campbell said.
He said both intravascular ultrasound (IVUS) and optical coherence tomography (OCT) are good supplemental imaging modalities to aid visualization for stent apposition and more accurate measurements. Campbell uses a Volcano IVUS system as his preference, because OCT takes longer to use.
Read the article “Role of Imaging in Bioresorbable Stent Procedures.”
Need for Precise Sizing and Catheter Movements
“The advantages of the robotic system play right into the need for precision when using the BVS,” Campbell explained. The Corpath has a millimeter-increment scale on the navigation screen, and its wire manipulation system enables a stable movement set by the operator in millimeter or sub-millimeter increments. He said this enables much more precise measurements and device delivery capability.
Campbell explained this is very important because of the Absorb’s key drawbacks — namely its very large stent strut size of 150 microns and its limited ability to be overexpanded. Another drawback is the discovery in trials that it has higher rates of stent thrombosis when used in 2.5 mm or smaller vessels. It is believed the poorer outcomes when compared to conventional metallic stents are due to the large size of the device’s struts, which obstruct blood flow.
For this reason, it is recommended that the Absorb not be used in vessels 2.5 mm or smaller.
It is also important for operators to keep in mind that vessel and stent sizing are very important to outcomes, Campbell stressed. This issue is compounded when multiple stents are required, because overlapping struts may cause significant disruption in blood flow. In cases where multiple stents are needed, he said the best technique is not to overlap them.
“So, you need to pay meticulous attention to vessel and stent sizing,” he explained. “The key to success is paying meticulous attention to positioning and technique.”
The need for more precise sizing, positioning, the difficulty in visualizing a non-metallic stent, the need for millimeter movements, and the fact that the Absorb is a newer device and operators are still learning to use it, make for longer cases, Campbell said.
“Most operators think they can do all this manually, but we are looking at 3-D anatomy on a 2-D screen that is constantly moving,” Campbell said. He also pointed to two studies he was involved in that compared visual measurements on angiography to measurements made with the robotic system. [1,2] The visual estimates were highly varied based on the operator looking at the images. Data show only 35 percent of the lesions measured visually were accurate compared to the Corpath system. Use of the robot also helped reduce stent usage by 8.3 percent because it did not underestimate lesion length.
“I use the robotic system a lot for measuring,” Campbell said. “Interventional cardiologists are not very good at measuring visually, and with the Absorb sizing is critical.”
He said the robotic system’s lead-lined cockpit also enables the operator to sit down without wearing lead aprons and it has a screen 10 inches in front of them, so it is much more ergonomic for these longer procedures. Campbell said the close proximity of the screen also eliminates the need to lean over the patient table to try and make out details on the overhead screen.
Read the article “Questions Remain on Future of Bioresorbable Stents.”
References:


 October 31, 2025
October 31, 2025 







