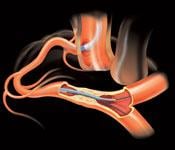
The key to treating chronic total occlusions is getting a wire across the lesion. The Terumo FineCross microcatheter is one of the main guidewires used to help cross these difficult-to-treat lesions.
Coronary chronic total occlusions (CTOs) are found in about one-third of patients who undergo angiography.(1) Most of these patients are referred to coronary artery bypass graft (CABG) surgery or medical therapy because these lesions are very challenging to treat using conventional percutaneous coronary interventional (PCI) techniques. However, a growing number of cardiologists are showing many CTOs can be crossed percutaneously if operators are willing to invest the time to learn new techniques.
“One of the biggest predictor of whether you get bypass surgery is dependent on whether you have a CTO or not,” said William Lombardi, M.D., FSCAI, medical director of cardiac catheterization laboratories at St. Joseph Hospital, Bellingham, Wash. “My guess is the number of bypass surgeries would go down if operators improved their ability to treat coronary CTO’s. This would also extend the number of patients receiving PCI instead of medical therapy to reduce ischemic burden, which is the biggest predictor of cardiovascular events.”
While about 1 million PCIs are performed annually in the United States, less than 50,000 of these procedures are done to treat CTOs, making up 3-5 percent of U.S. cases, Lombardi said. In Japan, where he says cardiologists are more aggressive and versed in treating CTOs, the rate is about 15 percent. In his own practice, Lombardi attempts PCI on all CTOs he finds that subtend viable myocardium, which is about 17 percent of his cases. Based on these numbers, he estimates about 100,000 CTO patients a year are not treated with PCI.
In the past, these lesions were seen as too difficult or dangerous to treat. Part of the reason interventionalists are reluctant is the lack of training and the shallow learning curve to master these procedures.
“It is not easy to do,” Lombardi said of learning these new CTO techniques. “Maybe not all operators should be doing this.”
The number of CTO cases may be too low for some lower-volume centers. Large numbers of cases are needed for an operator to become familiar and proficient with the techniques. He suggests at least one cardiologist per center take on these cases so they receive enough cases per year to become the resident CTO expert.
Long Procedures
The time it takes to conduct a CTO procedure is one deterrent to wider use of transcatheter treatment of these lesions. It took several years and many cases for Aaron Grantham, M.D., FACC, to bring his average CTO treatment time down to 90 minutes. He is a clinical associate professor of medicine at the University of Missouri Kansas City and Saint Luke’s Health System’s Mid-America Heart Institute in Kansas City, Mo. Many operators tell him they don’t want to invest that much time.
“That is a major hurdle for many operators,” Grantham said. “There is always one guy who stands up when I speak (at CTO technique training sessions) who says he does not have that amount of time to spend on one patient, due to the number of cases they have.”
Grantham and Lombardi are disappointed by these comments, because they believe many patients who are referred for bypass surgery or medical therapy could be successfully treated using PCI and experience better outcomes.
“Just because it’s long, just because it’s calcified is not a reason not to try. If there is a clinical indication, we will try,” Grantham said.
Tool to Cross CTOs
“There is no device that makes these procedures easier,” Grantham said. “All the current devices for CTO crossing are difficult to use and have a long list of dos and don’ts, which does not negate the fear factor of most cardiologists.”
While there are a large variety of interventional devices claiming features making them ideal for CTOs, Lombardi said the standard toolbox of the top U.S. CTO operators is relatively small.
“What really matters is if you can get a wire across the lesion,” Lombardi said. “It’s not so much devices, it’s technique. The key to any tool is using it properly.”
Microcatheters are very small sized hypotubes that are used for wire support and during a CTO attempt. Grantham and Lombardi said they use the Terumo FineCross MicroGuide catheter to approach highly stenosed, complex lesions, especially when they are dealing with tortuous vessels. Its stainless steel braided structure throughout the length of the catheter shaft and tapered design enhances tensile strength for increased reliability.
Abbott’s Asahi Tornus catheter is a favorite among CTO operators for crossing resistant lesions that cannot be crossed with a balloon dilation catheter. Its braided wire design and spiral-shaped tip can be screwed into occlusions, which helps pull the catheter forward without pushing it. Lombardi said this is important, since it is best to have CTO tools pull their way across lesions instead of being pushed, which may cause vessel damage. Tornus uses a braided stainless steel design for greater support and pushability, as well as flexibility for tortuous anatomy.
“The Tornus is a very capable device. There is not a day that goes by when we don’t use it,” said Patrick Whitlow, M.D., director of interventional cardiology at the Cleveland Clinic. Tornus should be used as a tool of first resort, because it offers the “push” needed for a guidewire to penetrate and tunnel through a CTO, he said.(2) For lesions that cannot be crossed with Tornus, Whitlow suggests the use of rotational atherectomy as a last resort.
Grantham said the Asahi Corsair is critical for retrograde approaches to CTOs. Like the Tornus, its braided wire design and scored tungsten tip act like a screw to help it pull its way through occlusions and small collateral channels. The ability to steer is another key component in the Corsair. Grantham and Lombardi use it to help traverse collateral vessels, allowing retrograde access to the distal CTO cap.
Grantham said there are several wires that must be part of the CTO toolbox. The Asahi family of wires offered in the U.S. by Abbott are ideally designed for tackling CTOs, which has put the company in a dominant position in the CTO market. These wires include the Fielder XT, Fielder FC, Miracle Bros, and Confianza wires by Asahi and the Pilot series of wires by Abbott. Grantham also frequently uses snares, which he said are needed for the retrograde approach.
“Keep your base of operations close to the end of the guidewires,” Lombardi suggests. This makes it easier to torque the wire and allows greater penetration and control, whether using the tools in an antegrade or retrograde approach.
New Coronary Tools
Many CTO tools were designed for peripheral leg vessels. BridgePoint Medical is developing two tools specifically for coronary CTOs — the Crossboss and Stingray catheters. The Crossboss spins to cross lesions. The Stingray balloon is flat so it can be inserted into the subintimal space, will align with the vessel and allow re-entry into the true lumen through one of three exit ports.
Lombardi participated in the FAST CTO trial to test these devices. He said these tools are scaled down to treat the smaller coronary vessels. The trial recently ended and Bridgepoint is expected to release preliminary results at TCT 2010. Lombardi said these tools are something to keep an eye on in the coming years.
The Stingray and Crossboss were cleared for use in Europe last fall.
New Skills, Training
Lombardi said there are no one-size-fits-all tools or skills to tackle CTOs. He said each lesion is different based on plaque composition, anatomy and length. He said the common PCI techniques do not apply to CTOs.
“Almost all of the skills we learn with doing CTOs are new,” Lombardi said. Since these cases are extremely varied, different skills may be required for each patient. He said this makes it difficult to teach these techniques to new CTO operators — even experienced cardiologists. A key issue with the training is that some cardiologists do not believe they need to learn new skills.
“You need to put your ego aside and admit you need to learn these new skills,” Lombardi said. “One of the most important things you can do is find a mentor to help you.”
Becoming a good CTO operator requires time to learn these skills. He added case volume is also important, because skills cannot be perfected with only a few cases per year.
“I would not recommend it to the guy who is only doing 50 or 60 interventional cases a year,” Grantham explained.
Only about 60 percent of CTOs are crossed using the standard antegrade approach. The lesion caps from this approach tend to be calcified, but Grantham said the retrograde caps are usually softer and easier to cross. This, combined with newer crossing techniques for harder caps, account for the improved success rates with retrograde CTO angioplasty. But, new skills are needed to navigate the smaller, tortuous collateral vessels to reach the far side, Lombardi said.
Bilateral Artery Access
CTO procedures usually require two sheaths, one in each leg, or each arm, so two diagnostic catheters can be inserted. Grantham said the use of two catheters is needed so contrast can be injected to help visualize the vessel before and after the CTO. Visualizing the distal target is critically important for success with the antegrade approaches.
“It’s another big hurdle that operators need to overcome,” Grantham said. “There seems to be so much reluctance to place another sheath and another catheter. They try to do a single vessel injection, but they can’t see their wires or the distal target vessel.”
For example, he said the vessel beyond a right coronary artery CTO often receives collateral perfusion from the left coronary arteries through the septum, from the left anterior descending artery, or from epicardial channels off the circumflex. A simultaneous contrast injection in both the right and left coronaries is needed to show the progress of a procedure, otherwise an operator may not know where they are or how far they have to go.
Knuckling Wires
The “knuckled wire” technique was developed by Lombardi as a way to push through CTOs without using a sharp end of a wire that can pierce the vessel wall. Grantham said the Fielder or Pilot wires work best for this method, which involves looping the wire around, so the blunt loop of the wire is used to push through the obstruction. The hydrophobic, polymer coating of these wires helps them slide along the outer lining of the vessel. Once across the occlusion, a Confianza or Pilot wire can be used to re-enter the true lumen.
Complications
The complication rate for treating CTOs is between 2-3 percent. “The biggest concern is perforation, but it’s not that common,” Grantham explained. Research indicates perforations occur in less than 1 percent of cases, usually by wires that exit the very distal portion of the vessel.
Another issue with CTO cases is prolonged patient radiation exposure due to procedures lasting from 90 minutes up to several hours. Grantham said imaging from one position causes burns, so he usually rotates the C-arm into different positions. He said use of collimation is the most effective way to reduce exposure to patients and operators.
2. Patrick Whitlow. Crossing CTOs session, Transcatheter Cardiovascular Therapeutics (TCT) 2008.



 November 14, 2025
November 14, 2025 







