MSHA has leveraged its enterprise imaging and reporting system to closely link its cardiovascular departments at multiple hospitals. This helps generate cardiovascular data analytics used to improve workflow and care.
Mountain States Health Alliance (MSHA), headquartered in Johnson City, Tenn., created a plan 10 years ago to improve its cardiovascular department through better IT infrastructure, applications like the hospital information system (HIS), electronic medical record (EMR), cardiovascular information system (CVIS), and better workflow efficiency and data analytics to run the department like a business. The health system also wanted consistency in care and data reporting from MSHA facilities that serve 29 counties in Tennessee, Virginia, Kentucky and North Carolina. Through use of its CVIS it was able to greatly improve workflow, cut reporting time, reduce critical results turnaround times with chest pain patients in the emergency department, and improve quality data reporting standards, including registry data transfer, throughput analytics, patient data mining, integration of appropriate use criteria (AUC) and adhering to meaningful use requirements for healthcare IT under the Affordable Care Act (ACA).
MSHA leveraged the data mining analytics capabilities of its Siemens syngo Dynamics CVIS, which uses structured reporting. The healthcare system used it to improve patient care, identify bottlenecks in hospital efficiency and improve door-to-balloon (D2B) times. MSHA created an enterprise imaging system by connecting all its departments and facilities through its HIS, CVIS and EMR systems.
“The enterprise mindset has had a major impact on our facilities and should be considered for any hospital that wants to improve its business,” said William Nottingham, RDCS, RCS, cardiovascular ultrasound and informatics manager at MSHA. “The enterprise element is very, very impactful. We can look across our healthcare system, see the data and identify areas where we need to make improvements.”
The ability to rapidly pull and analyze data in a transparent manner is crucial when making business and patient care decisions. “Transparency is very important and syngo Dynamics offers us this tool,” Nottingham said. “You need to know what is happening behind the scenes. We can look at numbers without crunching a lot of data. We can pull a report from last week or over the past five years for actionable data that is not based on my own gut feelings.”
Converting From Paper to EMRs
MSHA began its conversion from paper to electronic records in 2006 with the adoption of Siemens EMR and Siemens syngo Dynamics CVIS. “Our goal was to build a system-wide IT model and look at data not just at one hospital, but across the entire healthcare system,” Nottingham said.
The CVIS is now used at 13 hospitals and two outpatient diagnostic centers. However, it took longer to implement the reporting system in the cath labs, which still used dictation. The cath labs eventually went live, reporting within syngo Dynamics in 2011. Cath lab physicians had a major concern regarding structured reporting, which was their perception that the reporting process would take a longer time than just dictation. This fear proved to be unjustified. With the structured reporting process the need for transcription services was greatly reduced and the reporting content is now consistent and comprehensive. In fact, the reporting process is now faster than it was previously.
“Because our physicians were accustomed to using dictation, it took some time to implement this,” Nottingham said. “But we knew that once they converted to structured reporting, there would be positive gains in cath lab workflow and data collection.”
Today, all cath lab information since 2011 can be data mined, and report turnaround times have vastly improved. “We have seen more than a 50 percent improvement in turnaround times since implementing the structured reporting system,” Nottingham said. “We have seen major quality improvements since implementing the system. It was a matter of bringing all hospitals and physicians up to the same data reporting expectations, and giving them the tools to accomplish this.”
Sharing Data Across Departments
Faster reporting times and connectivity for all facets of the cardiovascular department now enable more streamlined communication of patient data with other parts of the hospital and referring physicians. The enterprise-wide data system also reduced or eliminated the need for repeat data entry. “The fact that we can now get the reports back to the EMR, the emergency department (ED), floor nurses and step-down units quickly has been a major driver for us,” Nottingham said.
All data entered into the CVIS is shared via the HIS. As reports are updated, the changes immediately become available on the HIS.
Sometimes identifying small changes can have a major impact. Heart failure is a major cause of readmissions, so MSHA decided to pull critical data for managing these patients into an area of patient records where it can quickly and easily be referenced. Nottingham said they pull the discreet ejection fraction (EF) values buried in echocardiogram reports and make them immediately available on the patient’s electronic health record.
“This has simplified the physicians’ work in regards to collecting patient data when trying to pinpoint a single piece of data from the patient’s echo report,” Nottingham said. “It has improved the process of ordering proper medications and managing the patient’s care.”
In addition, he explained, the CVIS offers immediate access to heart failure patients’ entire cardiovascular history going back several years, which offers a clearer picture of a patient’s condition to determine therapy.
Non-clinical interfaces to data include an automated inventory control system connected to MSHA cath lab reporting. As supplies and devices are used in each case, they automatically register in the inventory control system for billing. When inventory levels reach a preset amount, the system automatically bills and reorders the items.
Reducing STEMI D2B Times
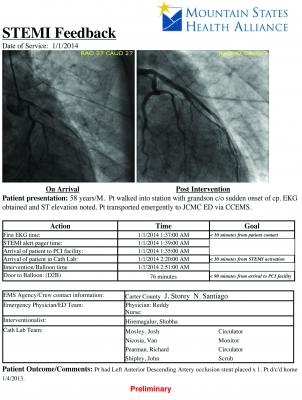
Another example of data sharing enabled by MSHA’s CVIS is the adoption of a ST-segment elevation myocardial infarction (STEMI) report. This has been leveraged to help D2B times at MSHA’s eight cath labs in three of its hospitals. Each hospital works closely with its emergency medical service (EMS) providers, starting with transmission of pre-hospital ECGs on all suspected STEMIs, and issues a report on all STEMI patients transported so EMS can see the impact of their work.
“We have seen a major increase in community satisfaction for STEMI patient care,” Nottingham said. “We wanted to let EMS, who bring the patients to us, know their work matters and they are helping save lives.”
MSHA built a STEMI report that includes all relevant, key stats on each patient, including arrival times, first ECG time, cath lab activation, time counts in the cath lab, pre- and post-intervention images, and patient post-procedural status. The patient data is anatomized and is sent to the ED, EMS and any other players involved with STEMI care so they can see the impact of timely care and how each link in the chain helps reduce D2B times. These reports show the performance of each level of the patient’s care and can show the quality of care by physician.
“Our door-to-balloon times have decreased as we have paid more attention to reporting the data,” Nottingham said. D2B averages fell from about 66 minutes in 2012 when the STEMI system was implemented, to less than 60 minutes today.
Greater Access for Referring Physicians
Traditionally, physician’s finalized invasive procedure reports had an expected turnaround time of 30 days to referring physicians. Patient care was able to continue through the use of handwritten physician progress notes and patient care plans; however, final case completion was a lengthy process.
Prior to use of the CVIS, referring physicians often faced a multi-day turnaround time for reports, due to logistical limitations of reading from VHS tapes. This has been significantly improved since the adoption of structured reporting and a CVIS system. As an example, Nottingham said echocardiography reports now have an average turnaround time of three to five hours. For echo reports, referring physicians get the complete document, and for invasive procedures they receive a case summary report.
“In most cases, we can get results back to the ordering provider the same day as testing, and that has been a big improvement to patient care,” he explained.
Speeding Throughput of Observational Patients
With growing concern over declining reimbursements and bundled payments, MSHA is concerned about how to best diagnose chest pain patients in the most cost-effective manner. Nottingham said the CVIS is used to monitor data for observational patients. “This patient population has become a major priority, and the analytics tools we use are very adaptable,” he said.
Data mining the CVIS identified issues with observational patient exam report turnaround times, which averaged 13-14 hours. “We identified this as an area that needed improvement and we now have gotten this down to six hours, which is a 50 percent reduction from what we were previously doing,” Nottingham said.
Data monitored includes exam report turnaround times and admissions to look for trends and ways to improve the management of these patients.
More Efficient Cath Lab Management
MSHA has six catheterization labs at its Heart Hospital at Johnson City Medical Center and one each at two other outlying hospitals. All of them use the same structured reporting forms so data can be compared at each facility or across the system. Management of the labs has greatly improved with the ability to data mine the information, and various performance reports are created with minimal effort. Data gathered helps determine the workload of each lab by day and week, peak usage times, types of procedures performed, report and patient turnaround times, orders entered after hours for emergency cases, supplies used for different types of procedures (electrophysiology, coronary peripheral, etc.), wait times and case split times when a diagnostic cath converts over to an interventional procedure. He said all of these reports were customized in-house.
Integrating the CVIS With Various Vendors
Interoperability is a key issue when installing a CVIS that needs to collect data from a large number of imaging and diagnostic systems, and the issues can be compounded when these systems are made by a multitude of vendors, or predate use of standardized Integrating the Healthcare Enterprise (IHE) integration profiles. However, Nottingham said they had few issues integrating their CVIS with multiple vendors’ equipment.
“The syngo Dynamics system has worked well, and I say that with a clear conscience,” he said. “We have not seen any deficiencies or downtime. The programming is pretty open and I think Siemens was ahead of the curve in making their software compatible with other vendors’ equipment.”
He said some software patches were needed and some of the older legacy equipment (including echo systems) simply did not support the data features included in syngo.
Customized Data Analytics
Nottingham’s advice on data collection is to start with a clean data set and think about what you will need to gather to make actionable decisions. This includes gathering data on all patients all of the time, not just on some reports, some of the time. “You need to choose good numbers and a good data metric that you can monitor, and you need to be prepared to do something about it,” he stressed.
Analytic reports can be created in-house, and all it takes is knowledge of how the system works, he said, adding that the vendor supplies templates that can be modified by the hospital. MSHA created standardized templates across its system, but customized each site’s reports with each hospital’s header and logo. Nottingham also has customized the templates to add new fields where MSHA wanted to gather data.
“It is truly customizable to my facilities,” Nottingham concluded. “We can create new data fields, report templates and analytic reports to support our changing needs.”
Improving quality of care, patient and clinician’s satisfaction and reducing cost are important objectives in today’s healthcare environment. Business and clinical analytics are essential to achieve this goal.
This case study was supported by an educational grant from Siemens Healthcare



 December 23, 2025
December 23, 2025