Image courtesy of Eko
Before opining on the future of cardiac health, I think it’s important to define what “cardiac health” actually is. If one searches the internet for the term, the result is a cornucopia of self-promotion and advertising. Yes, some of the content is helpful, but mostly these are pitches for an individual’s or group’s services. Not particularly useful, in my opinion.
For this article, I will define and divide “cardiac health” into two broad, separate categories: Cardiac disease prevention, and cardiac disease treatment. Generally speaking, modern healthcare systems are far too focused on the latter, which is understandable considering the high prevalence of cardiac disease with its associated morbidity and mortality. But treating established disease is the much more expensive choice and is really not sustainable. So, let’s discuss treatment first.
Cardiac Disease Treatment
One can think of disease treatment in two discrete steps or phases. The first is recognizing the disease, that is, diagnosis, and the second is management or treatment. For both of these phases, technology is making tremendous advances in improving diagnostic accuracy and treatment effectiveness.
Considering detection and diagnosis first, it’s important to realize that these are really exercises in pattern recognition. Looking at the X-ray, reading the ECG, asking specific questions during a history, assembling the findings of a physical examination — making a diagnosis from those is assembling and recognizing patterns. And machines are very good at doing that, from picking out cats in photographs, to breast cancer in mammograms, to murmurs in recorded heart sounds. And by layering on labeled data, machine performance steadily improves.
Of course, these machine algorithms aren’t perfect. But neither are humans. And unlike humans, machines work 24/7/365, they never fatigue, never need to take a break, and never have a bad day. Replacing humans with machines for diagnosing disease isn’t necessarily a bad thing, as long as we realize that machine diagnostic models work in a world of probabilities; that is, they never say with 100% certainty that something is or is not true. They output a likelihood that the diagnosis is correct. And here is where the human expert plays a role: When no one diagnosis the machine selects has a convincingly high probability. It is then that human intuition and experience can select the correct diagnosis.
But after the diagnosis is made, what about treatment? To the extent that medical therapy today has become protocolized and routine, machines can be trained to treat just as well as any human. Take for example closed loop insulin pumps that use a programmed routine to deliver insulin depending upon the readings of blood glucose taken from a continuous monitor. Or surgical robots that smooth human tremors so that highly magnified microsurgery can be performed more safely and precisely. Or monitoring systems that can alert physicians to critical changes in a patient’s physiological state such that immediate attention is required.
As long as the machine can be taught the rules (sometimes explicitly by the human, other times by itself as with deep learning from large, labeled datasets), the treatment rendered to the patient will be precise, unfailing and predictable. Having this function removed from the clinician actually frees the clinician to care for the patients who cannot be managed by routine or protocol, or who are failing and require experienced, human management. Overall quality of care improves, costs are reduced, and patient and clinician satisfaction is better.
In contrast to treatment, we should make every effort to increasingly focus on prevention. Why? Prevention is much less expensive than treatment. It reduces the overall burden of disease to society. It is simpler to implement. However, prevention takes significant time and effort up front, because it requires behavioral change rather than the seemingly simple “fix it now” treatments that come in a pill or a procedure. So how can we overcome those challenges to achieve what is much more worthwhile?
Cardiac Disease Prevention
Although we have known for many years of the risk factors that expose patients to cardiac disease, and of the salutary effect of controlling them, there simply has not been wide adoption regarding risk reduction. Here are some real life examples: Obesity is a growing problem.1 Exercise has not enjoyed wide adoption.2 Blood pressure control guidelines are tighter than ever, but patient compliance remains an issue.3 Why is this? Why do people ignore good advice, when it is within their grasp to control their fate?
I believe the answer is “inadequate touch.” What do I mean by this? Many studies have shown that the more contact patients have with their healthcare provider(s), the healthier they are.4–9 Regarding cardiac disease, the high-touch approach means that patients are more likely to alter their diet and their lifestyles in beneficial ways that prevent or forestall cardiac disease. Unfortunately, at present that is an unsustainable model. We simply do not have sufficient healthcare resources to keep after every single American, to ensure that they all follow a healthy lifestyle. Or do we?
I contend that we actually do have sufficient resources, but those are resources that will come in the form of technology. And we don’t need to reinvent the wheel. As of this writing, more than 80% of Americans, and more than 70% of people in the top 10 developed countries, have a smartphone.10 That is an astounding fact, and a straightforward path to our target. As the World Health Organization has stated, “Most cardiovascular diseases can be prevented by addressing behavioral risk factors such as tobacco use, unhealthy diet and obesity, physical inactivity and harmful use of alcohol. It is important to detect cardiovascular disease as early as possible so that management with counseling and medicines can begin.”11 So, we need to identify and control risk factors through technology, mainly the smartphone, and identify disease as early as possible (which was discussed earlier in this article).
Why am I dwelling on the smartphone? Have you ever noticed how much people use their smartphones? How they stare at them when they’re in the elevator? Walking down the street? Even at dinner with other people? In fact, the average mobile phone user opens her phone 69 times a day.12 Yes, the smartphone is the new opium of the masses. And if we put behavioral coaching software on people’s phones, it will be with them everywhere they go, all the time. They will see it and (hopefully) use it many times a day. Of course, it is not true that if we build it, they will come. Sophisticated attachment methods will be needed and are being actively explored and evaluated.13–15 But the end result must be, and likely will be, that we provide the high level of touch needed to maximize the likelihood that people achieve a healthy lifestyle and prevent cardiac disease.
This is not a new idea. Search the Apple App Store or the Google Play Store for “healthy lifestyle,” and you will be greeted by an uncountable number of apps — some based in science and adhering to accepted guidelines, others a little more dubious, but still plenty to choose from. One of the best is from the American Heart Association: My Life Check — an iOS app and an online interactive tool that encourages users to form healthy habits that have been shown to reduce the risk of cardiovascular disease. It helps users concentrate on controlling their blood pressure, controlling their cholesterol, reducing their blood sugar, increasing their activity, eating a healthy diet, losing weight and stopping smoking.

My Life Check is an interactive online tool that helps people assess and track their heart health information and gain a better understanding of their risk of heart disease and stroke.
Telehealth to Deliver Care
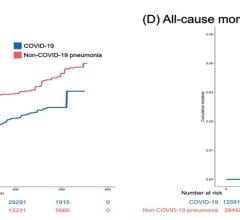
But beyond a healthy lifestyle and diet, what else can technology offer our patients that increases touch and cardiac health? One of the clearest lessons learned from the COVID-19 pandemic is not that “telehealth is here to stay,” but that telehealth can be truly effective for delivering care, and for keeping the physician-patient relationship alive and healthy. And these benefits apply not only to routine visits, but also to specialized applications of care such as cardiac rehabilitation.16
The challenge facing us now is how to increase the value of telemedicine beyond a simple video visit. This will come by putting medical grade, professional grade, internet enabled devices into patients’ hands. Leading the charge are devices like the Eko smart stethoscope and the Tyto remote otoscope that allow clinicians to remotely auscultate patients’ hearts, lungs and abdomen, and see inside the ear. More devices will surely come, with the aim of replicating the in-office visit.

The Tyto remote otoscope
By leveraging remote connectivity, patients should automatically enjoy increased access to care. Why “should,” and not “will?” Because we must overcome the significant inequity that exists regarding access to our infrastructure. For example, even though telemedicine visits have increased enormously during the COVID-19 pandemic, historically vulnerable populations still experienced much worse access to care.17 It wasn’t the technology, it was the access to it. We have the tools, but we need to get them into the hands of those who need it the most. Hopefully some of the many proposed bills to support increased access will be enacted, and we will see the benefit of this in the near future.18
Many will ask, “OK, but what about consumer-directed devices such as the Apple Watch and the Alivecor Kardia Mobile?” These devices do provide consumers with some useful information about their health, but because they are being used over-the-counter, without clinician supervision, direction or relationship, we are now starting to see some of the untoward effects such as unnecessary anxiety and testing.19 Although some of these shortcomings are being addressed by obtaining physician over-read of any readings via contracting, this actually circumvents the patient-physician interaction and leads to no lasting relationship; this is known to increase the risk of inefficiency, unnecessary and repetitive testing, and even increased medicolegal litigation.20 Certainly our society has moved toward the quick-hit type of encounter, but that thinking should not apply to our health care. Prevention is a marathon, not a sprint.
Technology’s Role in Cardiac Health
To summarize, the future of cardiac health will see technology play a very large role. From screening for disease using artificial intelligence-enabled tools, to helping the clinician manage disease by flagging problems and analyzing data, to preventing disease by promoting healthy lifestyles, to increasing access to care via remote patient visits, cardiac health is moving into the digital age. For some this change will be uncomfortable, but change always is. The benefits, however, will be well worth it.

Adam E Saltman M.D., Ph.D., is the Chief Medical Officer of Eko, a digital health company applying machine learning in the fight against heart and lung disease. Saltman obtained his doctoral degrees from Columbia University and subsequently trained in general and cardiothoracic surgery on the Harvard/Deaconess Surgical Service. He practiced cardiothoracic surgery until 2013 when he joined FDA as a Medical Officer in the CDRH Office of Compliance. In addition to his responsibilities reviewing manufacturer recalls, signals, and manufacturer communications, Dr. Saltman led CDRH’s cross-cutting policy revisions concerning benefit-risk, and corrections and removals. He also has developed methods that employ decision analysis tools to help FDA and industry minimize risk from medical device problems while maintaining access to effective devices. Dr. Saltman is a fellow of the American College of Surgeons, the American College of Cardiology, the American College of Chest Physicians, and the American Heart Association. He has published more than 100 peer-reviewed articles, served on editorial boards, conducted competitively funded research projects, completed advanced training in Health Informatics from the University of Illinois at Chicago, and is certified as a Quality Improvement Associate by the American Society for Quality.
 March 20, 2024
March 20, 2024