The Lumedx CVIS is an example of a system that can integrate data from across the cardiovascular service line into one location and eliminate disparate silos of information.
For any cardiology department planning to upgrade its cardiovascular picture archiving and communication system (cardiac PACS or CPACS), or cardiovascular information system (CVIS), the main questions that should be asked are related to integration and interoperability. These are key to leveraging health IT investments to achieve improved efficiency, help cut costs, and meet new regulatory mandates and reimbursement documentation requirements.
There are a handful of universal truths when it comes to new health information technologies (HIT). Primary among these is that new software systems should improve workflow, eliminate the need for separate workstations, connect all the disparate silos of patient data into one place, address all the ongoing requirements involved in healthcare reform, cut costs, and they should optimize patient care. Here is a list of 10 questions hospitals should ask vendors to help ensure the system they are purchasing addresses these needs.
1. What does your department need in a CVIS?
Prior to starting the search for a new CVIS, all the stakeholders need to first ask themselves what they need a new system to do. This discussion should include not only the various managers within the cardiology service line, but also nurses and techs who perform the bulk of the data entry tasks, and the hospital and healthcare system information technology (IT) administrators. Each of these stakeholders should come up with a list of what they need a new system to do. This might include a list of things they do not like or are unable to do with their current CVIS. IT staff would outline what they need from a CVIS to easily integrate into the overall hospital and healthcare system infrastructure. This may include requirements for integration into electronic medical records (EMR), hospital information systems (HIS), inventory management systems, PACS, patient portals, image and data sharing systems, or vendor neutral archive (VNA) systems.
2. Does the system need to meet all the required clinical functionality and reporting needs in a CVIS?
Interoperability across a hospital or health system is greatly simplified if the number of disparate systems that need to be connected are reduced. This includes minimizing the number of independent, standalone systems used in a service line. Look at what subspecialties need to be included in a new system’s functionality that may be operating on their own software systems outside the current CVIS. This might include electrophysiology (EP), coumadin clinics, and vascular or interventional radiology users in the cath lab. How well can a new system reduce the number of these standalone software systems? Or, how well can the new CVIS integrate with these systems if it cannot offer a comparable software solution? The new system should deliver coordinated cardiac care without the need to use different workstations, graphical user interfaces and sign-ons. Functionality in many cardiac departments need to include:
• Cardiac and peripheral catheterization (including pediatric);
• Electrophysiology;
• Hemodynamics monitoring and reporting;
• Echocardiography (including pediatric and fetal);
• Vascular ultrasound (including pediatric);
• Nuclear cardiology;
• Electrocardiogram (ECG)/stress/Holter management and reporting; and
• Ability to document newer procedures such as transcatheter aortic valve replacements (TAVR) and left atrial appendage (LAA) occlusions.
3. Will the new CVIS improve workflow?
New software systems should improve workflow and make it faster, not add extra steps or clicks that add time or additional potential points for data entry error. All information should be able to flow through the system without a lot of manual intervention so clinicians can complete reports faster, ensure full reimbursement, and enable consistent and accurate data for analytics analysis. This may include better mapping of how data should flow from the hemodynamics system into the proper documentation fields in cath lab reports. Some newer CVIS offer auto cross-checks to ensure all data fields needed to complete a report or registry filing are entered.
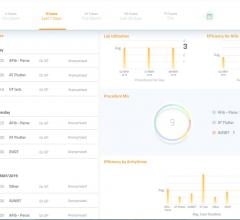
4. Does the CVIS system offer detailed analytics?
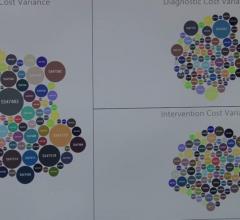
After hospitals implement fully digital patient records that integrate across departments, the next big push in HIT has been installing high-powered analytics software to datamine this information. Analytics in the past few years has moved far beyond simple dashboards to dedicated, complex, powerful data mining and interpretation software. Departments can now use analytics to better visualize bottlenecks in workflow, lost revenue sources, staff performance, inventory items used for different types of procedures or by physician, patient wait times, procedure times based on type or the doctor involved, report turnaround time, and the list goes on. Data-mining is also being used to identify trends in cardiac patient readmissions, ways to reduce door-to-ballon times and ways to cut costs. Analytics should be able to help monitor the usage of equipment, or adherence to guidelines or protocols. Advanced analytics also makes it very easy to track the number of cardiac cases brought to a hospital, or where referrals are coming from.
5. How can a new CVIS system save money?
Consolidation of data from a number of disparate systems for ECG management, nuclear imaging, echo, cath lab, EP and others into one place should immediately reduce the amount of staff time to find patient information. If a new system offers a lot of automation, such as auto-complete for specific report fields directly from an imaging or hemodynamics system, this can reduce turnaround times when completing post-exam or -procedure reports. This may enable doctors to perform more studies per day because they are not spending as much time putting together reports. Also, having immediate access to patient records across a department or hospital may help identify the last time a patient had a certain test done, which may prevent unnecessary or duplicated patient studies.
6. Does the Cardiac PACS offer structured reporting?
Structured reporting uses a standardized set of taxonomy selections to ensure everyone filing a report is talking about the same thing. In unstructured reporting, it is common for different terms or descriptions to be used that might mean the same thing, but this makes them difficult to use for data-mining or comprehensive analytics. Systems that offer structured reporting usually help increase efficiency and completeness of the data and allow reports to be immediately available after a physician signs off on them.
7. Is it better to use an EMR cardiology module or a dedicated, but separate, CVIS?
Healthcare systems may spend millions or billions on the purchase and deployment of an enterprise-wide EMR. Most of the larger EMR vendors offer cardiology reporting modules that just bolt on to their EMR and enable immediate interoperability. This creates a lot fewer headaches for hospital IT staff. However, the common complaint about these modules is that they are not as detailed in their reporting capabilities as needed by some subspecialties in the cardiovascular service line. They also often lack useful features or the robustness found on third-party CVIS. Since the electronic health record has become the master system of record, it is critical that the CVIS is well integrated with the enterprise EMR to avoid patient record gaps and to have the ability to generate analytics. If a standalone CVIS cannot integrate well with the hospital’s EMR, it will be difficult to justify its purchase to hospital administrators and IT staff.
One of the main challenges with the CVIS and EMR is the lack of discrete data flow between the two systems. If the hemodynamics system is native to a CVIS, there is more data exchange between CVIS and EHR, but this still requires customization. If a third-party hemo system is in place, the additional integration creates a barrier to discrete data exchange for items such as labs, medication, vital signs and utilized supplies, to name a few. In these cases, a static report is generated and the data is locked within a document. Procedure notes taken during a case provide richness to the patient record, and most of the time, these data remain in the hemo or CVIS due to the integration barriers.
There is logic to performing documentation and procedural reporting via a module in the EMR rather than establishing an interface from the CVIS to the EMR. Buyers need to look at the quality of the data being captured and if there are advantages of a full CVIS that will be worth the integration efforts. This will often boil down to whether data auto-populates the procedural reports with discrete, structured data and if the EMR module can meet the reporting requirements of all the service line CVIS users. Cardiology reports also need to be able to pull in images and/or waveforms from various sources to include in a final report. It is not a problem for the EMR to query an image archive for viewing relevant image data. The difference is that a CVIS ensures the discrete data in a report correlates as a presentation state on the procedural image. For example, if the measurement of a stenosis during the diagnostic portion of a cardiac catheterization is measured at 90 percent occlusion, a CVIS reflects this measurement in the report and likewise as a presentation state on the image. Measurements following an intervention adhere to the same workflow. Upon completion of the procedure, a cardiologist will often conduct final review of the report data for approval. At times, the pre- and post-procedural measurements are amended by the cardiologist. If the data fields are amended in the CVIS, the images immediately reflect the change to ensure both the image and the report are synchronized with the same information. If a cardiologist visualizes the report generated in the EMR module and pulls the images from a separate system to correlate, do post-procedural changes on the report trigger changes on the image? Can the EMR report module provide image object change management (IOCM) to ensure the report data matches the presentation state of the image data? This is a critical consideration as it is imperative that the report information perfectly matches the image presentation state. Also, there is the question of if an EMR module can deliver the numerous discreet data points needed to auto-populate cardiovascular registries. If not, this may require full-time clinical staff to complete registry forms for each case, adding overall costs to the department.
If a third-party CVIS is going to be purchased, the vendor should explain how its information will integrate with the hospital’s EMR or enterprise data management system. The majority of integrated CVIS solutions in the market offer a native short-term storage that is tightly integrated for DICOM structured reporting (DSR) exchange. In addition to the online CPACS or CVIS systems, most vendors now also offer a VNA. If an enterprise has already implemented a VNA for an enterprise imaging strategy, it is crucial to understand how the CVIS will integrate with the third-party VNA. IOCM certification, an Integrating the Healthcare Enterprise (IHE) standard, has become an accepted industry benchmark to ensure that image objects stay in sync as they are routed through various repositories.
8. Does the CVIS system allow greater data access for referring physicians and/or patients?
While expected turn-around times for final reports to referring physicians may have taken from a couple days to a month in the past, in the digital age the expectation is much faster. Today, modern computerized reporting systems have cut this time to a few hours. Faster reporting times and connectivity for all facets of the cardiovascular department now enable more streamlined communication of patient data with other parts of the hospital and referring physicians. Enterprise-wide data systems have reduced or eliminated the need for repeat data entry. Vendors need to map out how their systems can share images and reports digitally with referring physicians, whether it is through the EMR, HIS or a web-based remote viewing/sharing system.
Another consideration is how patients can access their reports, labs and images via web-based patient portals. These are becoming much more common to increase patient engagement, reduce the need to burn CDs or copy documents, increase patient involvement in their own care and to easily allow them to share their information with other doctors outside of the hospital network.
9. Does the CVIS integrate with other systems it needs to share data with?
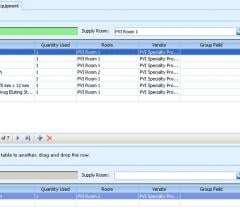
Moving beyond the EMR interoperability questions, is the CVIS capable of sharing both clinical and business data bi-directionally? There needs to be assurances that “work-around” processes will not be needed to interface with up- and downstream software systems that need to share CVIS data. These systems may include inventory management, billing, registry reporting (ACC, STS, radiation dose, etc.), enterprise clinical reference or clinical decision support, enterprise data analytics, XDS registries and health information exchanges (HIE). A high degree of integration diminishes the errors that accompany dual/manual entry of procedural information. From a business perspective, one should consider how procedural, diagnosis and other billing information flows dynamically into the billing system.
In addition, data from third-party imaging, diagnostic and monitoring systems in the cardiology department need to integrate with the CVIS. For example, advanced visualization and or analysis software may not be inherent to the CVIS, although the data produced by these systems needs to be incorporated into the CVIS and presented to clinicians for review and interpretation. This includes data from intravascular ultrasound (IVUS), 3-D/4-D echo, strain analysis, MIP/MPR features (e.g. curved, oblique, orthogonal MPRs) and quantification measurements.
10. Is the CVIS vendor product roadmap relevant to your organization’s strategy?
As a customer in the CVIS market, the procurement of the system essentially becomes a marriage, not a date. Thorough understanding of current features and functionality is critical, but equally as important is the vendor’s outlook on the CVIS market and healthcare as a whole. Healthcare is changing rapidly and the vendors are under ongoing pressure to stay agile and innovative. Is the CVIS vendor’s next set of functionality enhancements scheduled for release in line with your organization? If not, is the vendor willing to partner with your key stakeholders to collect and design specific system functions/tools that will address significant gaps in the following years? On the other hand, is the CVIS vendor releasing upgrades every four weeks, creating a support nightmare for your CVIS administrators? It is a fine balance in the growing healthcare field and the CVIS vendor partnership needs to start during the procurement process. A CVIS vendor’s ability to quickly turn around certain functionality and work closely with your needs will establish a strong bond with your key stakeholders.
Editor’s note: Val Kapitula, RT(R), PMP, CIIP, contributed information for this article. He is a healthcare IT consultant/partner at Paragon Consulting Partners.
Related Cardiovascular Information System Content:
Leveraging Cardiovascular Data to Improve Care and Efficiency
VIDEO: What to Look for in a New Cardiovascular Information System
Interoperability is Biggest Issue Facing CVIS/Cardiac PACS
Consolidation of Cardiology Data and its Integration Into the EMR
Newer Hemodynamic Monitoring Systems Address Need for Integration
Consolidating Cardiovascular Information Brings Care and Operational Benefits
Advanced Analytics Software for Cardiology
VIDEO: What to Look for in CVIS and PACS Workflow Efficiency
It Takes Two to Tango — A Common-Sense Approach to CVIS Initiatives


 February 15, 2022
February 15, 2022