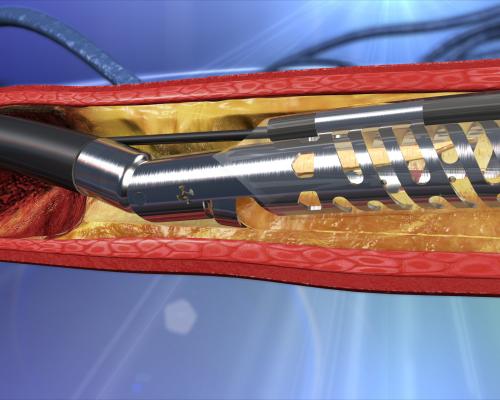
The Medtronic TurboHawk atherectomy system.
Due to poor outcomes from percutaneous transluminal angioplasty (PTA) ballooning of vessels alone, or of stenting in peripheral vessels, atherectomy has been adopted as a new therapy to improve treatment of peripheral artery disease (PAD) and critical limb ischemia (CLI). Atherectomy systems are used to remove heavy plaque burden from atherosclerotic lesions to prepare the lesion area for balloon angioplasty, with or without stenting. This debulking of lesions is often performed in vessels where plaque burden is especially heavy and difficult to treat with angioplasty, including chronic total occlusions and heavily calcified lesions. Heavy calcium prevents angioplasty balloons from fully expanding. Overexpansion of balloons to tackle tough lesions also can lead to barotrauma of the vessel.
Lower-extremity arteries (iliac, femoral, popliteal and tibial) are constantly exposed to torsion, lengthening and rotation during regular patient activities. These stresses are unique to the vessels in the legs and lead to higher rates of calcified atherosclerotic burden.[1,2] These movement stresses also cause stent fatigue over time, leading to stent fractures. Atherectomy offers an alternative to stenting and stand-alone angioplasty, or can aid in lesion prep to enable a maximum lumen diameter, especially in calcified lesions, for stenting.
Major Atherectomy Company Acquisitions
With growing interest in atherectomy, several companies have recently acquired systems to include in their peripheral interventional portfolios. Boston Scientific Corp. purchased the interventional division of Bayer AG for $415 million in May 2014. The transaction included the JetStream system, which is unique in that it uses a drill bit-like catheter tip and a set of foldout side-cutting blades to debulk lesions.
Medtronic purchased Covidien in June 2014 for $42.9 billion. This transaction involved Covidien’s entire interventional portfolio, including its TurboHawk and SilverHawk atherectomy systems.
In May 2014, Volcano Corp. acquired AtheroMed Inc., which gained U.S. Food and Drug Administration (FDA) clearance in January 2014 for the Phoenix Atherectomy System for PAD. Volcano paid $115 million for the company. The Phoenix uses a rotating, front-cutting element located at the distal tip of the catheter to shave material directly into the catheter. The debulked material is then continuously captured and removed by an internal Archimedes screw running the length of the catheter.
New Atherectomy Technologies Enter the Market
There have been a few recent FDA market approvals for new atherectomy technology.
In March 2016, Avinger Inc. received 510(k) clearance for an enhanced version of its Pantheris lumivascular atherectomy system for the treatment of PAD. The new version of the system features improved ergonomics, physician controls and manufacturability. The Pantheris is the first intravascular image-guided system, allowing physicians to see where they are guiding the catheter from inside the artery, using optical coherence tomography (OCT). The original device was cleared by the FDA in October 2015.
“Atherectomy is a proven treatment that relieves pain and restores blood flow, and Pantheris has been eagerly anticipated in the clinical community because it is a leap forward in atherectomy technology compared to what we have had in the past,” said Thomas Davis, M.D., of St. John Hospital and Medical Center in St. Clair Shores, Mich. “Now, for the first time, we are able to see exactly where we are removing the plaque, and are better able to leave the healthy artery alone. Clinical data suggests that the precision offered with Pantheris will have a lasting positive effect on patient outcomes. In addition, Pantheris visualizes the artery without requiring ionizing radiation. Thus, OCT has the potential to reduce physician and patient X-ray exposure, which is a concern for all clinicians performing multiple procedures.”
The safety profile and efficacy of the Pantheris was demonstrated in the VISION trial. The study included 130 patients who were treated with Pantheris and followed for six months. The study achieved its primary safety and efficacy endpoints and showed a target lesion revascularization rate of 8 percent, and no reports of vessel perforation, clinically significant dissection or late aneurysm resulted from Pantheris.
In April 2015, the FDA cleared the Cardiovascular Systems Inc. (CSI) 4 French, 1.25 Solid Diamondback 360 Peripheral Orbital Atherectomy System (OAS). Specifically, the clearance covers the company’s 145-cm-long, 1.25 mm Diamondback 360 Solid Crown, 4 French sheath-compatible and the modified 1.25 mm Diamondback 360 Micro Crown, 4 French sheath-compatible systems. Both devices offer a smaller profile and a more flexible shaft for improved ease of use. The use of smaller access sheaths can help reduce procedure times, enable quicker patient recovery and result in fewer procedural complications from bleeding.
In July 2015, the FDA cleared CSI’s ViperWire Advance Peripheral Guide Wire with Flex Tip for the Diamondback. The new guidewire provides improved flexibility, navigation and ease-of-use, particularly in hard-to-reach, tortuous vessels when treating arterial calcium.
The FDA cleared the Medtronic HawkOne directional atherectomy system and it was released commercially in April 2015. The HawkOne provides an enhanced cutting mechanism to more effectively treat the widest variety of PAD plaque.
Clinical Data Supports Atherectomy as Front-line Therapy
Recent clinical studies have shown atherectomy can be safe and effective as a front-line PAD therapy. Results from the DEFINITIVE LE study using the TurboHawk and/or SilverHawk systems demonstrated 95 percent limb salvage in patients with CLI, and 78 percent overall patency in claudicant patients at 12 months. The DEFINITIVE LE study is the largest atherectomy study conducted to date with independent, core lab analysis of the clinical outcomes.[1]
“The DEFINITIVE LE study provides confirmatory evidence based on 12-month, independent core lab adjudicated data on the use of directional atherectomy in treating a diverse, real-world group of patients with PAD,” said James F. McKinsey, M.D., FACS, Mount Sinai Hospital, N.Y., co-global principal investigator and lead author of the study. “The study enrolled 800 patients, making it the largest trial with independent, core lab analysis for atherectomy to date. Results of the study demonstrate high limb salvage, patency rates and diabetic outcomes. This further confirms the effectiveness and versatility of directional atherectomy in a wide range of vessel sizes and clinical presentations. Atherectomy is an important treatment option as the therapy leaves nothing behind in the body and preserves all future treatment options.”
The prospective, multi-center DEFINITIVE LE study enrolled 800 patients in 47 centers in the United States and Europe and included two patient cohorts: those with claudication and those with CLI. For the first time in an atherectomy study, DEFINITIVE LE also included pre-specified sub-group analysis comparing patency rates in diabetic and non-diabetic patients.
“The outcomes for patients with claudication reveal that in the scientific landscape, directional atherectomy is not only safe but effective to a similar degree as previous trials in the superficial femoral artery (SFA). Diabetic patients, who remain challenging for therapy due to their advanced and multi-level disease, have similar patency rates to non-diabetic patients with claudication when performing directional atherectomy,” said Lawrence Garcia, M.D., co-global principal investigator of the study and chief of interventional cardiology and vascular interventions at St. Elizabeth’s Medical Center in Boston. “These findings provide strong clinical support for the versatility of directional atherectomy in treating patients with diabetes, claudication and critical limb ischemia.”
Among patients with claudication, primary patency was 78 percent at 12 months. Notably, this rate did not differ between patients with diabetes (77 percent) and those without diabetes (78 percent) — the first such results to be shown in a prospective, powered analysis. Specifically for the SFA, the patency rates were 83 percent in lesions under 10 cm in the claudicant cohort.
CSI announced in November 2015 that the first patients were treated in its OPTIMIZE study, a European study evaluating the acute and long-term clinical outcomes of orbital atherectomy with adjunctive drug-coated balloon (DCB) angioplasty versus DCB angioplasty. Specifically, the study will look at patients with calcified below-the-knee (BTK) lesions. OPTIMIZE also will compare the economic outcomes between the patient groups.
Cardiovascular Systems Inc. shared three-year results from its pivotal ORBIT II study in a featured clinical research presentation at the 2016 Society for Cardiovascular Angiography and Interventions (SCAI) conference in May. The ORBIT II study evaluated the safety and efficacy of the company’s Diamondback 360 Classic Crown in treating patients with de novo severely calcified coronary lesions.[2]
“Using the coronary OAS to treat calcium prior to stent implantation delivers procedural success and durable long-term outcomes in these complex patients with severely calcified coronary lesions,” said Jeffrey Chambers, M.D., of Metropolitan Heart and Vascular Institute, Mercy Hospital, Minneapolis, who presented the data.
Effectiveness of Laser Atherectomy
The first large prospective study to examine the effectiveness of laser atherectomy in the treatment of femoropopliteal in-stent restenosis (ISR) found that the procedure combined with PTA was more effective than PTA alone. Findings of the EXCITE ISR trial were reported at the 2014 Transcatheter Cardiovascular Therapeutics (TCT) scientific symposium.[3] Laser atherectomy using the Spectranetics excimer laser vaporizes plaque and thrombus to help restore blood flow. The multi-center, prospective, randomized, controlled EXCITE ISR trial compared the safety and efficacy of laser atherectomy with adjunctive PTA to PTA alone in the treatment of patients with femoropopliteal ISR.
The primary efficacy endpoint was freedom from clinically driven target lesion revascularization (TLR) through six months of follow-up. The primary safety endpoint was major adverse events (MAEs) at 30 days, including all-cause mortality, major amputation in the target limb or TLR. Major inclusion criteria included ISR target lesions larger than or equal to 40 millimeters, vessel diameter between 5-7 millimeters, and Rutherford class one to four. The trial enrolled 250 patients at 40 clinical sites, randomizing them in 2:1 fashion — a total of 169 subjects were enrolled in the treatment arm (laser and PTA) and 81 patients enrolled in the control arm (PTA alone). Both groups were similar in baseline demographics and lesion characteristics.
Lesion length averaged 190 mm and more than 30 percent of patients presented with total occlusion. Compared to PTA alone, laser atherectomy with PTA demonstrated superior procedural success (93.5 vs. 82.7 percent, p= 0.02). Freedom from TLR at six months was 73.5 percent for the laser with PTA group compared to 51.8 percent for the PTA group (p < 0.005). The 30-day MAE rates were 5.8 percent for the laser with PTA group compared to 20.8 percent for the PTA group (p < 0.001).
“EXCITE ISR demonstrates that laser atherectomy devices used with PTA are superior to PTA alone in treating even the most complex lesions in patients with femoropopliteal peripheral artery disease,” said lead investigator Eric Dippel, M.D., from the Genesis Heart Institute in Davenport, Iowa. “The procedure leads to better outcomes than the current practice and significantly reduces adverse events when treating in-stent restenosis compared to PTA alone.”
Comparison Chart of Atherectomy Systems
This article served as an introduction for a comparison chart of atherectomy systems in our print issue. The chart offers an apples-to-apples comparison of specifications from various vendors at www.dicardiology.com/content/atherectomy-systems. To view the chart you will need a login, but it is free and only takes a minute. The vendors in the chart include:
• Avinger
• Boston Scientific
• Cardiovascular Systems Inc.
• Philips Volcano
Spectranetics and Medtronic did not respond to our questionnaire.
References:



 November 08, 2024
November 08, 2024