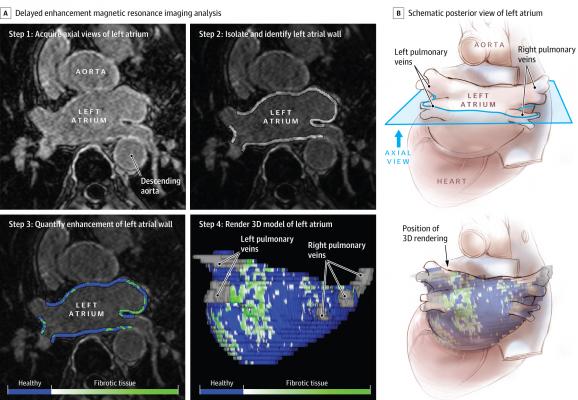
High-resolution 3-D delayed enhancement MRI of the left atrium can be used for quantification of fibrosis based on relative intensity of contrast enhancement The DECAAF study found this may help determine which patients will benefit from fibrosis ablation combined with PVI, and which ones are best served with the PVI.
September 28, 2021 — Image-guided fibrosis ablation in addition to pulmonary vein isolation (PVI) does not improve ablation success rates compared to PVI alone in patients with persistent atrial fibrillation (AF). This was according to the DECAAF II study intention-to-treat analysis presented in a Hot Line session the European Society of Cardiology (ESC) Congress 2021.[1]
However, in the as-treated analyses, covering low-grade atrial fibrosis with ablation lesions led to a significant reduction in atrial arrhythmia recurrence.
The multicentre DECAAF study previously reported that among AF patients undergoing catheter ablation, atrial tissue fibrosis estimated by delayed enhancement magnetic resonance imaging (MRI) was independently associated with the likelihood of recurrent arrhythmia.[2] The DECAAF II trial tested the hypothesis that imaging-guided fibrosis ablation in addition to conventional PVI is superior to PVI alone in improving ablation success rates in patients with persistent AF.
DECAAF II enrolled 843 patients with persistent AF from 44 centers worldwide. Participants were randomized to receive either PVI plus imaging-guided fibrosis ablation (intervention group) or PVI alone (control group).
All patients underwent late gadolinium enhancement (LGE)-MRI at baseline (before ablation) and approximately three months after. This imaging technique generates a 3D fibrosis map of the left atrium in which diseased or fibrotic tissue is shown in green and healthy tissue is highlighted in blue. Baseline images were used during the procedure in the intervention group to guide ablation of fibrotic tissue – operators were instructed to either cover or encircle the green areas on the images, i.e. the fibrotic tissue, in addition to PVI. Operators in the control group were instructed to only encircle the pulmonary veins, without adding additional lesions.
The three-month MRI evaluated the formation of lesions secondary to ablation. “These unique data provide us with the opportunity to better understand the effect of ablation on the left atrium and what parameters influence the formation of an ablation lesion,” said principal investigator Nassir Marrouche, M.D., of Tulane University School of Medicine, New Orleans.
“The results suggest that targeting atrial fibrosis in AF patients with low levels of fibrotic disease (less than 20%), may help improve ablation outcomes. In addition, the findings indicate that PVI should remain the mainstream ablation strategy in AF patients with high levels of fibrosis (more than 20%),” Marrouche said.
Participants were followed for the primary endpoint of atrial arrhythmia recurrence (including AF, atrial flutter, or atrial tachycardia) for 12 to 18 months. Atrial arrhythmia recurrence was detected through multiple ECG methods including 12-lead ECG recordings, Holter recordings, and a smartphone ECG device given to all patients after ablation.
The average age of participants was 62.1 years and 78.8% were men. Regarding atrial fibrosis levels at baseline, 98 participants (11.6%) had stage I (less than 10% of the total volume of the left atrial wall), 395 (46.9%) had stage II (10–20%), 281 (33.3%) had stage III (20–30%), and 69 (8.2%) had stage IV (more than 30%). Baseline fibrosis was predictive of AF ablation outcomes, especially at higher fibrosis levels, confirming the results of the initial DECAAF study.
The median follow-up was 12 months. The intention-to-treat analysis showed no statistically significant difference in the primary endpoint between groups in the total study population. Atrial arrhythmia recurrence occurred in 175 (43%) patients in the intervention group and 188 (46.1%) patients in the control group (hazard ratio [HR] 0.95; 95% confidence interval [CI] 0.77–1.17; p=0.63). In subgroup analyses, a trend was observed towards a lower rate of atrial arrhythmia recurrence in the intervention group for patients with stage I or II fibrosis at baseline.
As-treated analyses examined atrial arrhythmia recurrence according to the proportion of targeted and covered fibrosis (as assessed by the three-month MRI). There was a significant benefit of substrate ablation in patients with stage I or II fibrosis at baseline, with HR 0.839 (95% CI 0.732–0.961; p<0.05) for targeted fibrosis and HR 0.841 (95% CI 0.732–0.968; p<0.05) for covered fibrosis. However, there was no benefit of image-guided fibrosis ablation on atrial arrhythmia recurrence in patients with stage III or IV stage fibrosis at baseline.
The rate of complications, including post-ablation stroke, was higher in the image-guided ablation group but was mainly driven by patients with high levels of fibrosis at baseline.
Funding for the research came fromMedtronic, Boston Scientific, Biosense Webster, Abbott, Siemens, and GE Healthcare.
Disclosures: Marrouche reports having received consulting fees from Biosense Webster, as well as research funding from Abbott. Marrouche also reports having a family member as the CEO of Cardiac Designs.
Find more ESC late-breakering studies
References:

 May 22, 2026
May 22, 2026 







