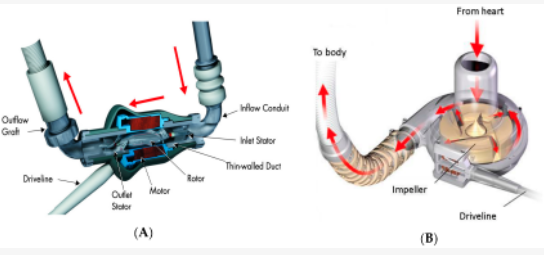
Pump housing and impeller design. (A): (left) Axial flow pump: HeartMate II LVAD (taken from Figure 2 in the HeartMate II left ventricular assist system instructions for use). (B) (right) Centrifugal flow pump: HeartWare assist device (taken from Figure 2 in the HeartWare assist device patient manual).
May 16, 2022 — Right heart failure (RHF) continues to be a major source of morbidity and mortality following left ventricular assist device (LVAD) implantation. Tricuspid regurgitation (TR) is frequently observed pre-operatively in patients undergoing LVAD implantation; and the presence of moderate or severe TR prior to LVAD appears to be associated with a high incidence of RHF during the first six months after the procedure.
Several retrospective studies have evaluated whether concurrent surgical correction of the tricuspid valve at the time of LVAD implantation can reduce post-operative RHF and improve outcomes. Most of these studies did not demonstrate a significant benefit for concomitant tricuspid surgery; however, these analyses are inherently limited by selection bias.
“We felt that this question had not been definitively answered, so we decided to perform a randomized controlled study on this topic,” said presenter Yuting Chiang, MD, New York Presbyterian/Columbia University Medical Center.
The purpose of the TVVAD trial was to determine the utility of tricuspid valve repair at the time of LVAD implantation for patients who present moderate or severe tricuspid regurgitation (TR). This study evaluated whether concurrent surgical correction of moderate or greater TR in patients undergoing LVAD implantation prevents post-operative right heart failure (RHF) compared to LVAD implantation alone. Chiang explained, “We used an adaptive trial design with a planned interim analysis to allow for early stopping of the trial for efficacy or futility and to allow for sample size re-estimation.”
Sixty patients with moderate or severe TR on pre-operative echocardiography were randomized to either LVAD implantation alone (No TVR, n=28) or LVAD implantation with concomitant tricuspid valve surgery (TVR, n=32). Randomization was stratified by pre-operative right ventricular (RV) dysfunction (none/mild vs moderate vs severe).
There was no significant difference in the primary outcome of the two arms. At six months, 46.43% of the TVR group and 43.75% of the No TVR group had experienced moderate to severe RHF. The study also looked at the incidence of all-cause mortality, atrioventricular block, major bleeding, prolonged mechanical ventilation, unplanned RVAD, and stroke and found no statistically significant difference. Based on this analysis, the trial has been discontinued for futility. Chiang said that they plan to follow-up with these patients and perform another analysis at one year to evaluate whether there are long-term benefits.
Muath Bishawi, MD, cardiothoracic surgery resident, Duke University, Durham, NC, and co-principal investigator for the trial, added “In our study, we focused on the primary endpoint, which was right heart dysfunction up to six months. Many other endpoints in the study, however, may be of interest to focus on for future trials. These may include late re-admissions beyond six months, quality-adjusted life years, and cost in hospital and long-term care.”
For more information: www.aats.org

 December 19, 2016
December 19, 2016