For decades, medicine has treated the electrocardiogram as a familiar, inexpensive and indispensable test, but also as relatively limited. We have relied on it to identify rhythm disturbances, conduction abnormalities, ischemic patterns and a handful of structural clues. That alone has made the ECG one of the most successful diagnostic tools in modern medicine.
What is becoming clear, however, is that we have been underestimating it. The transformation is not in the ECG itself, but in our ability to extract from it layers of information that lie beyond visual interpretation. With AI, the ECG is no longer just a tracing to be reviewed; it is a rich biological signal that can reveal hidden disease, sharpen risk assessment, and help determine what should happen next in care.
That is why ECG-AI matters. Not because it is novel, and not because every application of AI in medicine merits enthusiasm, but because it has the potential to turn a test that is already embedded in routine practice into a source of clinically useful insight precisely where earlier action can change the trajectory of disease.
That possibility is especially important in cardiovascular medicine, where disease often develops silently and declares itself only after meaningful damage has already occurred. By the time symptoms appear, patients may already have advanced dysfunction, lost opportunities for earlier treatment, or entered a more costly and difficult phase of care. At the same time, the tests that can confirm disease, especially cardiac imaging, are invaluable but inherently constrained by capacity, scheduling, cost, and the realities of follow-through in busy clinical systems. The result is a familiar gap in care: many patients who would benefit from earlier evaluation are not identified until much later than they could have been.
From Pattern Recognition to Clinical Decisions
The core promise of ECG-AI is straightforward: use patterns embedded in routine ECG data to identify patients whose risk is higher than it appears through conventional evaluation alone. These are not patterns a clinician is failing to notice. They are patterns that simply do not fit within traditional interpretation paradigms. AI models trained on very large ECG datasets can detect weak but reproducible signal relationships associated with ventricular dysfunction and other forms of cardiovascular disease. The result is not a diagnosis in isolation, but a more informed starting point for clinical decision-making. The key question is not, “How impressive is the model?” but, “What does it enable a clinician to do?” That is where the field either becomes clinically meaningful or remains an academic exercise.
A useful ECG-AI tool should not merely classify risk; it should help determine the next appropriate step. That may mean ordering an echocardiogram, escalating follow-up, reassessing management or referring a patient for more specialized evaluation. In other words, the value is not in pattern recognition for its own sake. The value is in changing the timing and precision of care.
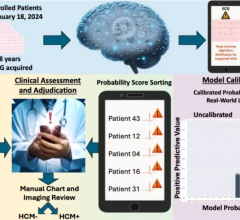
We are already seeing what that can look like. One case that has stayed with me, from the institution that invented ECG-AI, involved a 35-year-old asymptomatic man undergoing evaluation after a family member’s unexpected death. His ECG was interpreted as normal, but an AI algorithm flagged him as high risk for low left ventricular ejection fraction. Follow-up echocardiography showed an ejection fraction of 18 percent, and he was ultimately diagnosed with familial dilated cardiomyopathy.
That is not an argument that AI should replace clinicians. It is the opposite. It is an argument that clinicians deserve better tools, especially when disease is silent, confirmatory testing is finite, and time is always in short supply. The human interpretation was reasonable in its typical context. The problem was that conventional interpretation had reached its natural limit, while the ECG still contained more information than was being used.
That is why I see ECG-AI not as a replacement for clinical judgment or work, but as a force multiplier for it.

Untapped Adoption Potential of ECG
Of course, none of this means adoption is easy. One of the biggest gaps when talking about AI in healthcare is assuming that technical performance is the hard part and implementation is secondary. Health systems do not adopt algorithms. They adopt workflows, governance models, operational tradeoffs and new patterns of clinical behavior.
That is especially true for ECG-AI, where the barrier is often not interest but organizational readiness. Health systems have to decide who owns oversight, whether to partner with a vendor or build internally, how results will appear inside existing ECG workflows, which patients should be prioritized first, and whether downstream echocardiography and specialty capacity can absorb the patients newly surfaced. IT teams are already stretched thin, and reimbursement is still evolving, so these decisions are being made under both operational and financial uncertainty.
There is also a paradox that comes with success. If ECG-AI works, it will identify the right patients at the right time who merit follow-up, but the concern is that it will add pressure to already-constrained services. In practice, the opposite is true. ECG-AI identifies which patients truly need costly follow-up testing rather than a simple preventive measure, directing resources where they are genuinely needed. The answer is not to avoid earlier detection, but to embrace it intelligently, starting with defined use cases, targeted populations and workflows that allow scarce confirmatory resources to be used more effectively.
Intentional, forward-leaning adoption matters, and it is ultimately a question of institutional commitment and ownership. Health systems must take responsibility for driving transformational change at the same pace as innovation and real-world clinical behavior. Broad enthusiasm is important, along with an organizational commitment to innovation that does not compromise governance, workflows or patient outcomes. That discipline is what brings validated technology to every clinician who can act on it in real time.
Validation is equally important. Health systems are right to demand evidence that a model performs reliably across diverse populations and care settings. But I would go one step further: performance metrics alone are not enough. Beyond what is required for FDA clearance, additional retrospective studies reporting Area Under the Curve (AUC), sensitivity, specificity, or PPV still do not answer the questions that clinical leaders ultimately care about. Did the technology improve decision-making at the point of care? Did it lead to better targeting of confirmatory testing? Did it change who was diagnosed, when they were diagnosed, and what happened after that?
The EAGLE trial points in that direction. In a large prospective randomized real-world study involving 22,641 patients and 358 primary care clinicians, ECG-AI improved how efficiently low ejection fraction was surfaced in practice. That kind of evidence matters to adopters not because it adds another performance statistic, but because it begins to answer the operational question that ultimately drives uptake: what changes once the model is actually deployed?
Conclusion
Looking ahead, the significance of ECG-AI is broader than any single use case. It offers a path toward more proactive cardiovascular care by extracting earlier signals of hidden risk from a test already embedded across hospitals, clinics, and increasingly ambulatory settings. As ECG acquisition becomes more distributed, the ability to derive clinically meaningful insight from those signals will matter even more. Few technologies combine the ECG’s familiarity, low friction, scalability and reach. If rigorously validated and thoughtfully implemented, ECG-AI could become one of the more equitable forms of advanced diagnostics precisely because it builds on infrastructure medicine already has, rather than requiring entirely new pathways to be built from scratch.
To me, that is the real shift. We are moving from an era in which the ECG was valued mainly for what clinicians could directly see, to one in which it can also reveal latent risk that would otherwise remain hidden. The question is no longer whether routine ECGs contain more information than we have historically used. They do. The question is whether health systems are prepared to act on it.
The right response is neither hype nor hesitation, but disciplined adoption: validated tools, clear clinical purpose, thoughtful integration and a willingness to act before silent cardiovascular disease declares itself too late.

Dr. Samir Awasthi is vice president of clinical research at Anumana. He has been with Anumana since its inception in 2021 and with Anumana's parent company, nference, since 2019.
Partnering closely with Mayo Clinic, Dr. Awasthi plays a pivotal role in advancing a pipeline of AI-enabled software medical devices to detect and predict disease with unprecedented precision. His work includes designing and overseeing clinical studies that demonstrate the safety, effectiveness, and utility of ECG-AI, as well as clinical strategy with regulatory agencies, medical societies and healthcare payors.
Dr. Awasthi obtained his BS and MEng in Physics and Biomedical Engineering, respectively, from MIT, followed by an MD-PhD from the University of California, Davis, where he completed doctoral research at the NSF Center for Biophotonics Science and Technology (CBST). He furthered his clinical training at Harvard Medical School, where he also conducted neuroimaging research that leveraged data science and machine learning.

 May 20, 2026
May 20, 2026