
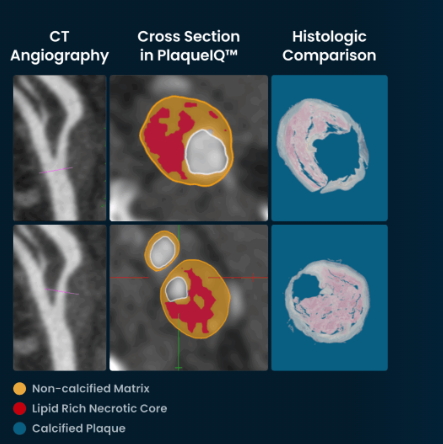
PlaqueIQ is trained and validated on ground-truth histology, providing physicians with comprehensive patient, vessel and lesion-level plaque composition and quantification data.
For decades, cardiology has evaluated coronary artery disease (CAD) largely through the lens of luminal stenosis, or the degree to which plaque narrows a vessel. This approach originated with invasive angiography and continues to shape both invasive and noninvasive imaging paradigms today. However, a growing body of evidence suggests that luminal narrowing alone does not fully reflect the underlying biology of coronary atherosclerosis or the mechanisms that lead to acute coronary events.
The central challenge facing clinicians is well recognized. Many myocardial infarctions arise from plaques that were previously non–flow limiting, often demonstrating less than 50 percent luminal stenosis before the event.1 This observation has prompted increasing interest in approaches that extend beyond the measurement of stenosis.
Advances in coronary CT angiography (CCTA) and computational image analysis have expanded the ability to evaluate plaque within the vessel wall. These developments have enabled more detailed assessment of plaque burden and characteristics beyond luminal narrowing. Among emerging approaches, methods that incorporate validation against histologic data are being explored as a means of better aligning imaging findings with underlying plaque biology.
Limits
Historically, stenosis severity has been the dominant metric for evaluating CAD. This focus is understandable, as angiography directly visualizes the vessel lumen, making narrowing the most readily measurable parameter. While guideline-driven and clinically validated, stenosis-based assessment has limitations. Luminal narrowing is not synonymous with plaque instability.
Atherosclerotic plaques develop within the arterial wall and may expand outward through positive remodeling. As plaque accumulates, the vessel can enlarge to preserve luminal diameter, allowing substantial plaque burden to exist even in the presence of a mild narrowing.
In addition, plaque composition is not directly correlated with the degree of stenosis.1 The risk of plaque rupture is influenced by biological and structural characteristics within the lesion, including lipid-rich necrotic core, fibrous cap thickness, inflammation, intraplaque hemorrhage, microcalcification, and arterial remodeling.2 Plaques with these features may be prone to rupture even when luminal obstruction is limited. As a result, stenosis alone provides an incomplete representation of cardiovascular risk.
Plaque Characterization
Noninvasive CCTA has expanded the ability to evaluate coronary atherosclerosis beyond simple stenosis measurement. It enables visualization of plaque within the vessel wall and supports assessment of overall plaque burden and composition.1
A commonly used approach to plaque characterization relies on Hounsfield unit (HU) attenuation thresholds. CT-derived attenuation values are used to approximate plaque components such as lipid-rich tissue, fibrous tissue and calcium. While this method has clinical utility, it represents an indirect approximation rather than a direct measurement of tissue composition.
Several factors complicate the relationship between attenuation values and true plaque characteristics. Threshold ranges for different types of tissue overlap, and attenuation values are influenced by scanner parameters, reconstruction techniques, contrast concentration and physical imaging effects such as beam hardening and partial volume averaging. As a result, similar tissue components may display variable attenuation values across imaging conditions.
In addition, the spatial resolution of CCTA limits the ability to directly visualize microscopic structures. Features such as thin fibrous caps or microcalcifications may fall below the resolution of a CT voxel, resulting in measured values that reflect a mixture of adjacent tissue types rather than a discrete component.
Taken together, these limitations indicate that attenuation-based classification provides a useful but simplified representation of plaque composition.
The Challenge
Plaque vulnerability is influenced not only by the presence of specific components but also by their spatial organization within the lesion. Structural characteristics such as necrotic core size, fibrous cap thickness and the relationship between calcium deposits and surrounding tissue may affect mechanical stability and rupture risk.
Attenuation-based approaches primarily classify voxels according to density and therefore provide limited insight into these structural relationships. In addition, biomechanical factors, including wall stress and interactions between plaque geometry and blood flow, contribute to plaque behavior but are not directly captured by attenuation values alone.
As a result, current approaches to plaque characterization describe composition in a relatively simplified manner and may not fully capture the complexity associated with plaque instability
Clinical Consequences
The clinical implications of plaque characterization remain an area of active study. Patients with nonobstructive coronary disease on CCTA are often managed conservatively based on current standards of care. However, it is well established that some acute coronary events arise from lesions that are not severely stenotic at the time of imaging.
This underscores a broader limitation: current imaging approaches may not fully capture the biological features associated with plaque instability. As a result, stenosis severity alone may not fully reflect underlying plaque risk.1
While advanced plaque characterization techniques are being developed to address this gap, there is currently no established guideline-supported role for their routine use in predicting or preventing clinical events. Accordingly, their potential impact on patient management remains to be determined through prospective study.
Histology as a Reference Standard
Because imaging techniques infer tissue composition indirectly, validation against histology remains important. Histology provides direct visualization of plaque components using established staining techniques and microscopic analysis and is widely regarded as a reference standard for characterizing atherosclerotic tissue.
Histologic analysis enables identification of lipid-rich regions, fibrous tissue, calcium, and inflammatory elements at micrometer-scale resolution. While tissue preparation may introduce artifacts, histology offers a detailed representation of plaque composition and serves as a foundation for evaluating the accuracy of imaging-based methods.
Applying Histology to Imaging
Ground-truth histology refers to the process of comparing imaging-derived features with corresponding histologic findings from tissue samples. By examining how imaging signals relate to directly observed tissue composition, investigators can better understand the strengths and limitations of different imaging approaches.
These comparisons can inform the development of computational models that attempt to identify imaging patterns associated with specific plaque characteristics. In the context of CCTA, such efforts are aimed at improving the alignment between imaging-derived measurements and underlying plaque biology. However, the reproducibility, standardization and extent to which these approaches can be applied reliably across clinical settings remain an area of ongoing investigation.
Quantification Versus Estimation
Another important distinction in plaque analysis is the difference between qualitative estimation and quantitative measurement. Traditional approaches often rely on descriptive categories such as mild, moderate, or severe plaque burden, which may vary between observers.
Quantitative methods aim to measure plaque characteristics using defined numerical metrics. Examples include total plaque volume and the volume of specific plaque components. These approaches may allow for more reproducible assessment and facilitate comparisons across imaging studies.
Although the relationship between specific quantitative measures and clinical outcomes remains under investigation, objective measurement represents a step toward more standardized evaluation of atherosclerotic disease.
Clinical Implications
Despite ongoing advances, the integration of detailed plaque characterization into routine clinical practice remains limited. Current guidelines continue to emphasize stenosis severity, ischemia testing, and traditional cardiovascular risk factors for clinical decision making.
Advanced plaque assessment may provide additional information about atherosclerotic disease beyond luminal narrowing. It has the potential to offer a more detailed description of plaque composition and burden. Whether such information improves risk stratification or meaningfully alters clinical outcomes has yet to be established.
In patients with nonobstructive disease or multiple lesions of similar severity, more detailed plaque characterization may offer insights into disease heterogeneity. However, the clinical significance of these findings, and how they should influence management, remain areas of active investigation.
An Evolving Field
The field of plaque imaging continues to evolve as advances in CCTA, computational modeling, and image analysis expand the ability to evaluate coronary atherosclerosis. At present, these developments are best viewed as part of an ongoing effort to better understand plaque biology rather than as established tools for guiding clinical care.
Future progress will depend on continued technical refinement, cross-platform validation, and prospective studies evaluating the relationship between imaging-derived plaque characteristics and clinical outcomes. As this work advances, plaque imaging may contribute to a more nuanced understanding of coronary artery disease, complementing existing approaches rather than replacing them.

Dr. Robert Pelberg is s Senior Vice President of Medical Affairs at Elucid. He is board certified in cardiovascular disease, cardiac CT angiography, nuclear cardiology and echocardiography. He previously served as a clinical cardiologist and advanced cardiac imager at The Christ Hospital Heart and Vascular Institute in Cincinnati, Ohio. He is a fellow of multiple professional societies, including the American College of Cardiology, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography.
References
-
Naghavi M, et al. From vulnerable plaque to vulnerable patient. Circulation. 2003;108:1664-1672.
-
Van Veelen A, et al. Detection of vulnerable coronary plaques using invasive and non-invasive imaging modalities. Journal of Clinical Medicine. 2022;11(5):1361.
-
Motoyama M, et al. Plaque characterization by coronary computed tomography angiography and the likelihood of acute coronary events in mid term follow up. Journal of the American College of Cardiology. 2015;66:337–346.
-
Williams MC, et al. Low attenuation noncalcified plaque on coronary CT angiography predicts myocardial infarction. Circulation. 2020;141:1452-1462.

 June 18, 2026
June 18, 2026 







