
Novadaq's CO2 laser system being used to create a channel in the myocardium to promote angiogenesis in infarct tissue.
Transmyocardial laser revascularization (TMLR or TMR) was introduced in the late 1990s as a method to offer relief to patients with incapacitating angina that were poor candidates for other procedures such as coronary artery bypass graft surgery or balloon angioplasty and stenting. The basis for the procedure is use of a laser to bore small holes from the ventricle into the myocardium, allowing blood to flow directly into the heart muscle without the need to travel through blocked coronary arteries. The belief is that this process helps enable angiogenesis.
Although it provided significant relief of the symptoms of angina in the majority of patients, it fell out of favor due to concerns about inconsistent data on perfusion improvement.
Due to the growing rates of obesity, type 2 diabetes and other conditions associated with metabolic disorder that can weaken veins, the subset of patients with severe coronary artery disease and angina who are not amenable to balloon dilation or coronary artery bypass grafting is becoming substantial. The growing need for alternative therapies and a more thorough investigation of TMR brings this therapy back into play. Careful culling of the data surrounding TMR shows that modality is very important, and correct technique improves results and decreases risks. Thus I have found that TMR performed with a carbon dioxide (CO2) laser to be very effective in this subset of difficult-to-treat patients.
Distinguishing Between Laser Modalities
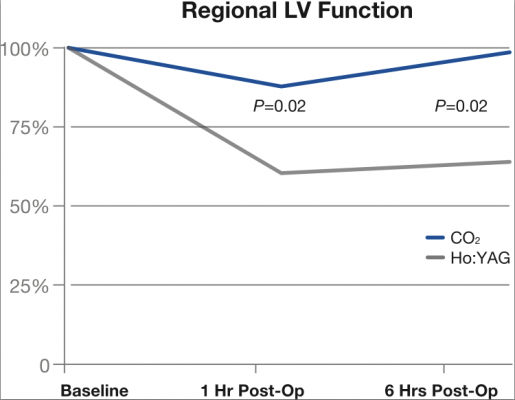
There are two primary laser types in use today with TMR — CO2 and holmium yttrium aluminum garnet (Ho:YAG) lasers. A number of large-scale studies combine the use of these two distinct lasers, providing an overall picture of TMR treatment that is less than ideal. However, when the data is separated, TMR using Ho:YAG is associated with impairment of left ventricular function in the immediate post-operative period and tissue damage, resulting in significantly impaired myocardial blood flow.[5, 7] Neither of these issues has been observed with TMR with a carbon dioxide laser, and 72 percent of patients showed significant improvement in the symptoms of angina.[4]
Comparisons of the two laser modalities show that Ho:YAG lasers create a zone of structural and thermal damage that is 3.5 times greater than the carbon dioxide laser, resulting in 5.7 times more volumetric tissue damage.[5] This additional tissue damage significantly impairs the left ventricular function as well as myocardial blood flow in the immediate postoperative period.[5] Neither of these impairments are observed with the carbon dioxide laser.[5] See Charts 1 and 2
The long-term efficacy of TMR with the carbon dioxide laser is also confirmed. In a study of 78 patients with severe angina not amenable to conventional revascularization, the average angina class was significantly improved from 3.7 + 0.4 at baseline to 1.5 + 1 at one year post-TMR with the carbon dioxide laser, which persisted for five years or more.[2]
With growing positive evidence for TMR with a carbon dioxide laser, the discussion has evolved to the mechanics of how it works. While this is an ongoing process, evidence supports the idea that a carbon dioxide laser promotes the enhancement and release of vascular endothelial growth factors in the cells, leading to angiogenesis.[3] In addition, the carbon dioxide laser increases vascularity, and high-resolution magnetic resonance (MRI) and ultrasound imaging show that this improvement persists over time.[4] This improvement in vascularity post-carbon dioxide TMR has been demonstrated to provide improved perfusion and cardiac function clinically[4], whereas the Ho:YAG laser has not been shown to improve perfusion or cardiac function.[4] This disparity led to studies which demonstrated denervation of cardiac tissue may play a role in angina relief post-Ho:YAG TMR.[3, 4]
Identifying Eligible Patients
It is important to clarify that even with the improved outcomes and risk profile seen when performing TMR with a carbon dioxide laser, it is still not a procedure for all angina patients. TMR is still reserved for those patients with a very difficult clinical picture. I perform TMR with the carbon dioxide laser in two ways: as a stand-alone procedure or in combination with coronary artery bypass surgery. As a stand-alone procedure, patient characteristics include an ejection fraction >30 percent, reversible ischemia, angina +3-4 and no segments of myocardium amenable to coronary bypass surgery. Patients must also be able to demonstrate to have reversible ischemia with sole therapy.[6] Operative mortality is similar to the results of coronary artery bypass grafting when these criteria are followed.[1]
Patients eligible for combination therapy have angina pectoris +1-5, at least one section amenable to coronary bypass surgery and demonstrable ischemia on a stress test.[6]
At my hospital, we have performed TMR with the carbon dioxide laser on more than 50 patients in the past two years and have compiled all data from these patients into a common databank. As the referring cardiologist considers TMR as sole therapy as a last-resort modality, it was employed for only a small percentage of patients. The majority of these patients received TMR in combination with coronary artery bypass surgery. The outcomes have been very good, and this coincides with other international studies that did focus solely on TMR with the carbon dioxide laser. Continuing to collect this data and sharing it with colleagues is the only means of educating cardiologists and other professionals on the merits of TMR as sole therapy.
The Future
Studies are currently underway to analyze the benefit of combining extracellular matrix and stem cells with TMR, and outcomes are positive.[4] It is possible that injecting emulsified extracellular matrix or stem cells around the channels created by TMR can regenerate new myocardial cells in an area of previous infarction or improve function in areas of ischemic cardiomyopathy by improving perfusion. The hope is that someone bedridden with Stage 4 angina can improve to a Stage 2 and be able to lead a relatively useful life. However, the tissue damage and inflammatory response subsequent to TMR performed with the Ho:YAG laser limits the success of this combination therapy.
Difficult cardiac patients with multiple complications are on the rise, and modalities are needed to treat them. Recurring symptoms, repeat hospitalizations and rising pharmacologic prices are combining to raise the cost of treating these patients. TMR is a good alternative that provides immediate and sustained relief for these patients, and may have even greater potential when combined with regenerative therapies.
References:
1. Frazier OH, March RJ, Horvath KA for the Transmyocardial Carbon Dioxide Laser Revascularization Study Group. “Transmyocardial Revascularization with a Carbon Dioxide Laser in Patients with End-Stage Coronary Artery Disease.” N Engl J Med 1999; 341:1021-1028.
2. Horvath KA, Aranki SF, Cohn LH, et al. “Sustained Angina Relief 5 Years After Transmyocardial Laser Revascularization With a CO2 Laser.” Circulation 2001; 104:1-81-1-84.
3. Horvath KA. “Mechanisms and results of transmyocardial laser revascularization.” Cardiology. 2004;101(1-3):37-47.
4. Horvath KA. “Transmyocardial laser revascularization.” J Card Surg. 2008 May-Jun;23(3):266-76.
5. Kadipasaoglu KA, Sartori M, Masai T, et al. Intraoperative arrhythmias and tissue damage during transmyocardial laser revascularization.” Ann Thorac
Surg. 1999;67:423–31.
6. Bridges CR, Horvath KA, Nugent WC, et al. “The Society of Thoracic Surgeons practice guideline series: transmyocardial laser revascularization.” Ann Thorac Surg. 2004 Apr;77(4):1494-502.
7. Hughes GC, Shah AS, Yin B, et al. “Early postoperative changes in regional systolic and diastolic left ventricular function after transmyocardial laser revascularization: a comparison of holmium:YAG and CO2 lasers.” J Am Coll Cardiol. 2000 Mar 15;35(4):1022-30.




 May 28, 2026
May 28, 2026 







