
March 5, 2023 — Providing medications for chronic diseases—for example, cholesterol-lowering, blood pressure and diabetes medications—free of charge for three years did not have a significant impact on serious health outcomes associated with those conditions among low-income seniors in Canada, according to a study being presented at the American College of Cardiology’s Annual Scientific Session Together With the World Congress of Cardiology.
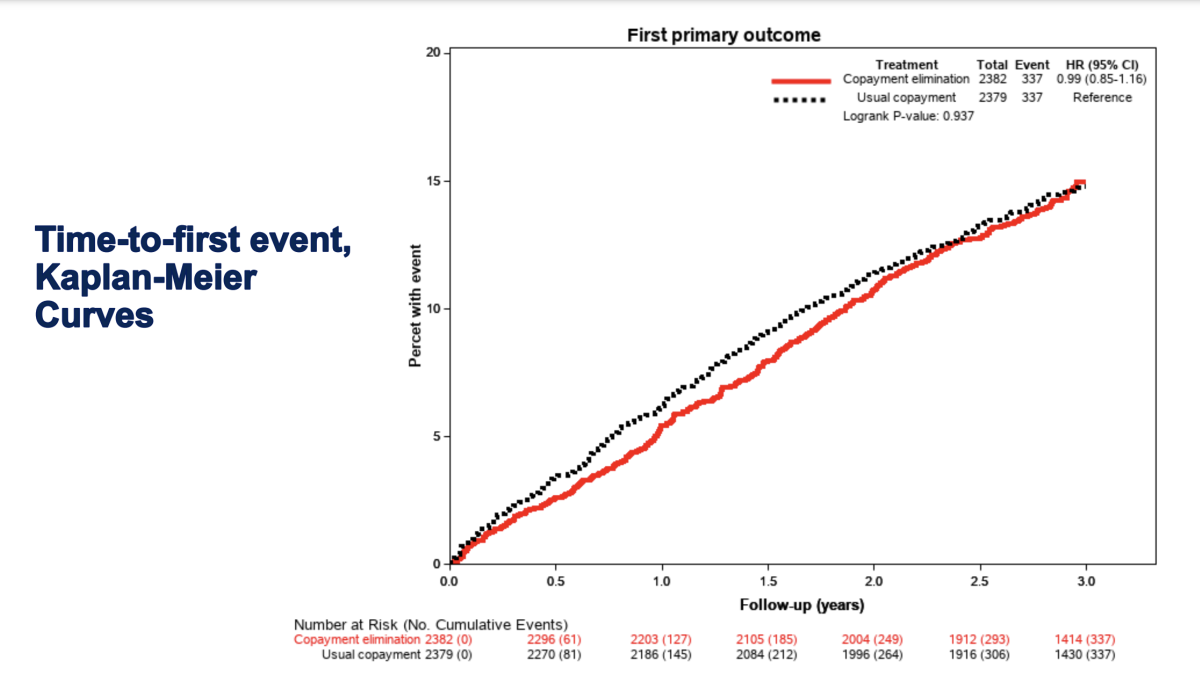
The trial, conducted in Alberta, Canada, brought an average savings of 35 Canadian dollars (CA)—or $26—per month for participants in the intervention group, but eliminating this level of copayment did not show any significant benefits in terms of the study’s primary endpoint, a combined rate of death, heart attack, stroke, coronary revascularization (procedures to open blocked arteries) or hospitalization for cardiovascular-related conditions such as heart failure, coronary artery disease or diabetes.
“Our findings suggest that the current policy in Alberta, Canada, is probably reasonable; even though it leaves people with some costs, they’re not overburdensome in this population,” said Braden Manns, MD, professor of medicine at the University of Calgary in Canada, and the study’s senior author. “Most experts in health policy will actually be quite surprised by this. It’s a negative trial but still one that we can learn a lot from.”
Available medications can significantly reduce the risk of cardiac events among people with chronic diseases such as heart disease, diabetes and chronic kidney disease. However, studies estimate that about 1 in 8 people with such conditions cite cost as a primary reason for not continuing preventive medications, and people of lower socioeconomic status tend to have worse outcomes from chronic diseases than wealthier people.
The researchers sought to determine whether eliminating all patient-borne costs could increase medication adherence and thereby improve outcomes among low-income seniors, a group considered particularly vulnerable to poor cardiovascular outcomes. The study enrolled 4,761 people aged 65 and over with an annual household income below CA$50,000 ($37,400). All participants were at high cardiovascular risk as determined by a combination of diagnosed chronic conditions and/or risk factors such as smoking, high blood pressure and high cholesterol.
For half of the participants, all medication copays were eliminated for 15 classes of medications known to help prevent heart attacks, strokes and other forms of vascular disease or slow the progression of chronic kidney disease. The rest of the participants continued to be charged medication copays as usual under the universal public pharmaceutical insurance plan for seniors, which is 30% of medication costs, to a maximum copay of CA$25 ($19) per prescription.
After a median of three years, the results showed no significant difference between groups in terms of the study’s primary composite endpoint. There was also no difference in terms of quality of life or total health care costs. However, participants without copays were slightly more likely to take their medications as prescribed for several medication classes. The researchers did not identify any subgroups of patients who were more likely to benefit from the elimination of copayments based on demographic or health-related factors.
Several factors could explain why the intervention had no effect, including that the average cost savings to participants was more modest than expected. Researchers said that eliminating copayments may have a bigger impact among people who would otherwise bear a higher cost for medications, such as those who lack health insurance.
They also said that study participants had a relatively high rate of medication adherence at baseline and a lower rate of cardiac events than anticipated. Multiple reasons aside from costs may also influence a person’s ability to access medical care and keep up with preventive medications, Manns said.
“It’s not necessarily that cost isn’t an issue, but low-income people are facing many, many barriers, and cost is only one piece of the puzzle,” he said.
Although the findings suggest the current copay structure in Alberta, Canada, is not overly burdensome for low-income seniors who have access to universal medication insurance, researchers said further studies could help elucidate whether a similar intervention might have more of an impact among other groups of people, such as those who are uninsured or those living in the U.S., where the average person spends $1,500 per year on prescription drugs.
The trial incorporated a second intervention to assess whether patient education and support could improve outcomes. The two interventions did not affect each other, and the findings from the educational intervention part of the study will be reported separately.
This work was supported by Alberta Innovates-Health Solutions, the University of Calgary Clinical Research Fund and the Canadian Institutes of Health Research through a Foundation Grant.
This study was simultaneously published online in the journal Circulation at the time of presentation.
For more information: www.acc.org

 April 02, 2026
April 02, 2026 







