
Image: Getty Images
Cardiovascular disease (CVD) is a serious global health burden that encompasses a broad group of diseases that affect that heart and vessels such as coronary artery disease, stroke, hypertension and peripheral artery disease. Another class of cardiovascular diseases that have received a lot of attention in the last decade are rare CVDs (RCD) that affect few people and include conditions such as Fabry disease (FD), cardiac amyloidosis (CA) and hypertrophic cardiomyopathy (HCM).
RCDs in general were once neglected aspect of pharmaceutical industry; however, regulators are incentivizing developers to pursue unmet needs. As a result, new drug targets are increasingly discovered, and rare disease research is now receiving significant attention and investment from pharmaceutical companies. Mavacamten (Camzyos), for example, is a first-in-class, FDA-approved cardiac myosin inhibitor used to treat adults with symptomatic NYHA Class II-III obstructive hypertrophic cardiomyopathy (oHCM). The drug has been shown to improve functional capacity and reduce obstruction, often decreasing the need for surgical procedures. More recently, a second drug in the same class (cardiac myosin inhibitor), Aficamten (Myqorzo) received regulatory approval for the same indication. This is great news for people with hypertrophic cardiomyopathy that had few treatment options until now.
Hypertrophic cardiomyopathy, with estimated prevalence of 1 in 200 to 500, is a disorder of cardiac myocytes characterized by cardiac hypertrophy and myocardial fiber disarray disproportionate to loading stimuli (e.g., hypertension or aortic stenosis). This severe hypertrophy is often associated with a small LV cavity and a decrease in LV relaxation and compliance, which contributes to underlying diastolic dysfunction.
Fabry disease, a rare, monogenic X-chromosome-linked lysosomal storage disorder, is a multisystem disease with frequent misdiagnoses and significant diagnostic delays that adversely affect patient outcomes. The prevalence of FD is around 1 in 40,000 to 1 in 117,000 in the general population. Cardiomyopathy in FD includes progressive left ventricular wall thickness, ventricular dysfunction, myocardial ischemia, arrhythmias and valvular heart disease. Severe microvascular dysfunction is the primary underlying mechanism for myocardial ischemia in the absence of coronary artery disease. From a cardiac perspective, the main diagnostic challenge is distinguishing FD cardiomyopathy from other forms of unexplained LVH.
Cardiac amyloidosis with prevalence of fewer than 5 per 10,000 people, is characterized by the extracellular deposition of misfolded proteins (Amyloid) in the myocardium, causing cellular injury and impacting cardiac function. The deposition of abnormal proteins results in a restrictive and/or infiltrative cardiomyopathy characterized by increase in left ventricular thickness. Without treatment, it leads to progressive heart failure and, ultimately, death.
Biomarkers
Biomarkers play an important role in assessment of disease states, serve as objective indicators of normal and abnormal biological processes and provide useful clues about health. Identifying a biomarker that, if modified, say by a novel drug, should correspond to clinical improvement that ideally should be assessable qualitatively and quantitatively. Medical imaging modalities such as cardiac MR (CMR) imaging, provide a non-invasive way to assess cardiovascular disease and longitudinally evaluate treatment response in clinical trials. Moreover, due to lack of ionizing radiation, rapid imaging capability and superior soft tissue contrast, CMR is widely considered to be the gold standard for assessing heart structure and function. As a result of significant enhancements in hardware and software technology and maturing of acceleration strategies, the imagers now can implement advanced MRI methods, resulting in an emergence of novel and innovative CMR imaging biomarkers.
A typical CMR acquisition is performed on 1.5T or 3.0T MR scanners, consists of a series of structural MRI scans in a acquired as a cine series (images acquired in a cardiac cycle) that allows the clinician to review morphological information of the heart and vessels. Post acquisition, data is temporally reordered based on synchronization with retrospective ECG and presented as a continuously acquired time series (cine series). These series of images are used for morphological review of the atrial and ventricular chambers, valves and perform quantitative assessment of chamber volumes, wall and inter ventricular septal thickness. Left ventricular (LV) thickness is an important parameter required for evaluation of LV hypertrophy, a common structural finding in HCM, CA and FD. In addition, use of contrast agents, called GBCA or Gadolinium based Contrast Agents, are formulations of Gadolinium (atomic number 64) injected intravenously and can be used in conjunction with morphological imaging to enhance visualization and characterization of cardiac tissue.
Late gadolinium enhancement (LGE) technique has been shown to be very useful for detection of fibrosis and infiltration, and risk stratification in cardiomyopathies. LGE images are typically acquired after a delay of 10–15 minutes post intravenous administration of GBCAs and demonstrate fibrosis and infiltration as regions of high-signal-intensity (bright pixels against dark background) due to increased uptake and delayed washout of GBCA (hence the delay in acquisition).
These regions can be further analyzed by performing Region of Interest (ROI) analysis by drawing contours to extract metrics such as area/volume, signal intensity and dynamic wash-in wash-out information using analysis software. LGE is present in almost half of FD patients and typically involves the basal and mid inferolateral myocardium in about 75% of these patients. About one-fourth of FD females can develop LGE without LVH. Echocardiography, another useful imaging technique based on ultrasound technology, can miss 50% of the early-stage cardiomyopathy cases in females; however, CMR is able to detect majority of these cases. Therefore, the assessment of myocardial fibrosis by CMR is crucial in the screening and staging of FD, especially in female patients who may not meet conventional LVH criteria early on by echocardiography.
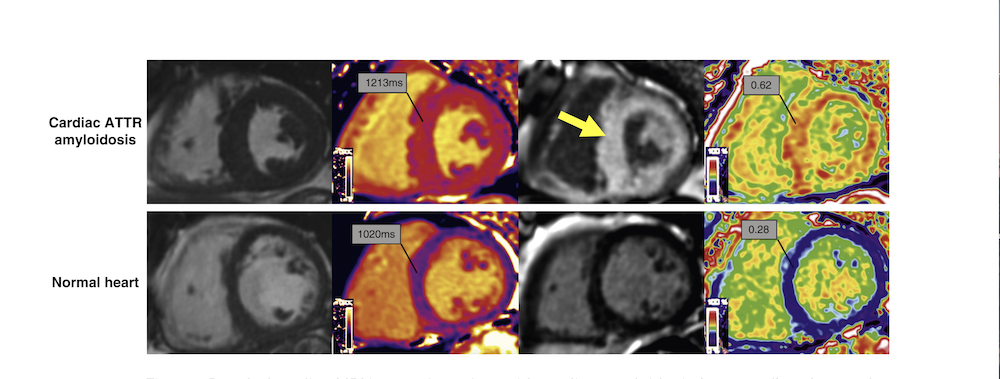
In CA, the expansion of extracellular volume resulting from deposition of abnormal amyloid fibril in the myocardial extracellular space is accurately visualized using LGE imaging. In HCM, LGE by CMR can both clarify the diagnosis and aid in risk stratification. Accumulation of GBCA in LGE imaging is seen in areas with expansion of extracellular space due to either edema or fibrosis resulting in increased signal intensity on T1 weighted imaging. In approximately 50% patients with HCM LGE has been noted and is commonly described as patchy and mid-myocardial within segments of maximal hypertrophy. The presence of LGE is associated with an increased risk of adverse outcomes for patients with HCM. In CA, LGE reflects both amyloid deposition in the myocardial interstitial space and subendocardial ischemic changes (fibrosis) are associated with microangiopathy. LGE has almost pathognomonic distribution in CA; Subendocardial LGE is more prevalent in a subtype of CA called Amyloid Light Chain (AL) CA while transmural LGE is more prevalent in Transthyretin-mediated amyloidosis (ATTR). LGE has been noted to be a significant predictor of mortality both in AL and ATTR.
CMR parametric mapping techniques such as T1 mapping, T2 mapping and Extra Cellular Volume (ECV) provide useful insight for assessment of diffuse fibrosis in CA, FD and HCM. T1 mapping technique quantifies the heart muscle's T1 relaxation time pixel-by-pixel, creating color-coded maps to assess tissue health. T1 relaxation time is measured in millisecond (ms) in each pixel in the myocardium and is a fundamental property of heart tissue that changes with pathology.
As a parametric map different colors represent different T1 values, allowing for precise quantification, unlike standard MRI contrast images. Parametric T1 mapping is typically performed in combination with LGE imaging, acquired before and after injection of GBCA (with and without contrast agent). One of the key properties of GBCA is to modify T1 values of tissues and any changes in T1 values (depends on the concentration of GBCA in the tissue) can be captured on parametric maps. ECV, a measurement of the size of the extracellular space, is calculated from native (pre-contrast) and contrast enhanced T1 values of myocardium and blood as well as patient’s hematocrit. ECV is elevated in amyloidosis and other infiltrative diseases, due to the expansion of extravascular space from amyloid deposits but in their absence, it is a biomarker for myocardial fibrosis.
In LGE imaging, initially native T1 values are reduced but later there is pseudonormalization in the areas of enhancement, allowing reliably differentiation of FD from other causes of LVH. While ECV values are normal in FD as it is an intracellular storage disease, as cardiomyopathy progresses, an increase in ECV values may be visible in areas of myocardial fibrosis. Measurement of myocardial deformation and mechanics by strain and strain rate analysis on CMR is an emerging tool for the quantitative evaluation of global and regional cardiac function in cardiomyopathies.
During the cardiac cycle, the myocardium (globally or locally) shortens, lengthens, thickens, and rotates; this deformation is referred to as myocardial strain, follows application of stress and is measured as change in the tissue between relaxed and contracted states. Due to complex motion of the myocardium, owing to its shape and varied orientation in different myocardial muscle fiber layers, deformation can be categorized as longitudinal strain (along long axis), circumferential strain (along short axis) and radial strain (towards center of ventricular cavity). Implementation of techniques such Feature tracking-CMR (FT-CMR) using current scanner technology is very feasible.
The technique is highly accurate for myocardial strain analysis in cardiac diseases, especially the assessment of LV global longitudinal strain (GLS) in LV hypertrophy has excellent reproducibility. GLS is significantly reduced in cardiac amyloidosis compared to Fabry’s disease and hypertrophic cardiomyopathy. In addition, global radial strain (GRS) is significantly reduced in Fabry disease and GLS impairment correlates with GL3/Lyo-GL3 elevation, thus having the potential in detection of early cardiac involvement.
Cardiac MRI
Cardiac MRI has come a long way since the humble beginnings of the early days of imaging when imaging of the beating heart was complex and images generated had significant blurring due to motion. CMR is now increasingly used in cardiology clinical trials for patient stratification, longitudinal monitoring of disease progression and assessment of response to therapy. Novel CMR biomarkers such as LGE, ECV and GLS measurements have enhanced our knowledge of pathophysiology of CVRDs, wider array of biomarkers to test treatment response and leverage them as key endpoints in cardiovascular rare disease trials.
Another equally important aspect of using novel imaging biomarkers in clinical trials is operationalizing the application of this technology in multi-centric setup. Moreover, rare disease clinical trials have unique challenges related to availability of a small pool of subjects, making it imperative that every procedure performed during visits including imaging be performed optimally to avoid any loss of data.
Ensuring integrity of imaging data from multi-centric clinical trials relies on various factors, including a well-aligned imaging modality, robust imaging acquisition standards, appropriate image interpretation, and use of well-thought-out central reads. Site-to-site variation can impact data collection; sites may use different scanners or staff with varying levels of experience. Defining the CMR image analysis strategy early, selecting CMR imaging experts based on appropriate experience and qualifications, providing standardized training, and implementing ongoing quality monitoring are essential to ensure imaging data tracks with regulatory expectation.
References
1. Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75, Erratum in J. Cardiovasc. Magn. Reson. 2018, 20, 9. Cardiovascular Imaging (NASCI)." Journal of cardiovascular computed tomography 10.6 (2016): 435-449.
2. Tower-Rader A, Kramer CM, Neubauer S, Nagueh SF, Desai MY. Multimodality Imaging in Hypertrophic Cardiomyopathy for Risk Stratification. Circ Cardiovasc Imaging. 2020 Feb;13(2).
3. Umer M, Kalra DK. Cardiac MRI in Fabry disease. Front Cardiovasc Med. 2023 Feb 2;9.
4. Rajiah PS, Kalisz K, Broncano J, Goerne H, Collins JD, François CJ, Ibrahim ES, Agarwal PP. Myocardial Strain Evaluation with Cardiovascular MRI: Physics, Principles, and Clinical Applications. Radiographics. 2022 Jul-Aug;42(4):968-990.
Rohit Sood, MD, PhD is vice president, Medical Imaging and Histopathology, at Perceptive Imaging. For more information, please visit www.perceptive.com.

 June 12, 2026
June 12, 2026 







