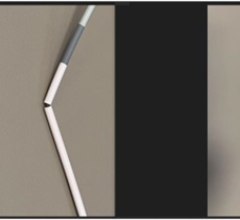
Figure 1. Serial coronary angiograms of the representative case treated with shockwave intravascular lithotripsy.
Over the last decade, there have been considerable developments in procedural techniques and technology facilitating the treatment of complex coronary artery disease (CAD). These were developed due to increasing burden of complex CAD encountered by interventional cardiologists as a consequence of an aging population who have greater burden of comorbidities. However, percutaneous coronary intervention (PCI) of calcified lesions continues to be one of the most challenging interventions, for which the optimal remedy remains elusive. It is expected that the burden of calcified CAD will increase over the next decades due to increasing patient longevity, therefore effective treatment for these lesions is vital.
Calcified lesions are associated with procedural failure and pose numerous challenges including device delivery, damage to the drug-eluting polymer, and impaired stent expansion and apposition, all of which is associated with adverse impact on PCI outcomes. Adequate lesion preparation is needed to minimize calcified CAD prior to PCI. Traditionally, this has been attempted with cutting/scoring balloons, high-pressure balloons and coronary atherectomy (rotational and orbital). However, use of these methods is limited due to risk of complications, degree of technical difficulty, operator experience or lack of sufficient evidence. Furthermore, these may not be effective on all calcified lesions, for example they have limited efficacy in treating eccentric, thick or deep calcifications. In these lesions scoring/cutting and high-pressure balloon angioplasty is limited in its ability to modify calcified lesions. Specifically, balloon dilatation of eccentric calcium results in expansion bias towards the non-calcified segment of the artery. In thick, deep, or concentric calcification it is unable to exert required force to liberate vascular compliance. Rotational atherectomy is effective in selectively ablating superficial calcium, with limited impact on deep or thick calcium that results in limited vessel expansion. Moreover, due to the mechanistic action of each device these can be associated with serious complications including slow/no-flow phenomenon, excessive vessel dissection, or perforation.
Shockwave intravascular lithotripsy (IVL) is a novel device that may be utilized in patients with calcified lesions. The technology gained European CE mark in May 2017 for coronary arteries. It currently has U.S. Food and Drug Administration (FDA) approval only for calified peripheral arteries, which it gained in June 2017. It is an innovative approach for treating calcified lesions that has the potential to allow interventional cardiologist tackle even the most challenging calcified lesions without serious complications experienced with traditional devices. Below is an outline of the technology behind IVL, the clinical trial data, its technical methodology, our real-world experience, and its potential role in the future.
Watch the VIDEO "How a Lithoplasty Balloon Shatters Calcified Plaque in Arteries With Ultrasound."
Watch a VIDEO interview "Breaking Up Calcified Lesions Without Vessel Trauma."
Technology Behind Intravascular Lithotripsy
Shockwave IVL is a novel device that delivers localized pulsatile sonic pressure waves, modifying calcified lesions in a safe and reproducible manner. The mechanism is leveraging electrohydraulic-generated lithotripsy to produce high-speed sonic pressure waves that pass through soft tissue to selectively disrupt calcium. The concept adopted is similar to urologic extracorporeal lithotripsy, but IVL differs by expressing a focal effect with ultra-high energy. IVL is designed specifically for vascular applications with the technology producing unfocused energy that creates a localized effect only within the vessel.
Shockwave Lithoplasty Clinical Data
The Disrupt Coronary Artery Disease (Disrupt-CAD) study is a prospective multicenter, single-arm study enrolling 60 patients with severely calcified lesions treated with shockwave coronary IVL. The main inclusion criteria of the lesions were severely calcified lesions in a native coronary artery with ≥50 percent diameter stenosis and >32 mm length. The primary performance endpoint was clinical success defined as a residual diameter stenosis <50 percent following stenting without in-hospital major adverse cardiovascular events (MACE: composite of cardiac death, myocardial infarction or target vessel revascularization). The primary safety endpoint was freedom from MACE through 30 days follow-up.
The study demonstrated compelling safety and performance results. Shockwave IVL treatment was highly effective in facilitating the delivery of stents and reducing restenosis. Stent deployment was performed in 100 percent of the patients with reduction in residual stenosis to less than 50 percent in all patients despite more than 90 percent of patients having heavily calcified lesions. There were no major intra-procedural complications including perforation, embolization, slow-flow or no reflow and a low MACE rate out to 6 months (8.5 percent). Consistent, reproducible luminal gain was also achieved. The clinical success rate was achieved in 57 (95 percent) patients, limited only by 3 (5 percent) asymptomatic non-Q-wave MI. IVL catheter delivery and treatment at the target lesion was successful in 59 (98.3 percent) patients. The primary safety endpoint of 30-day MACE rates was achieved. There were no cardiac deaths, Q-wave MIs or target vessel revascularizations during this time period.
Technical Methodology of Shockwave IVL
The Shockwave IVL system consists of a catheter that houses the emitters and is enclosed in an integrated angioplasty balloon mounted on a rapid exchange system, shockwave generator and connector cable. The balloon should be well prepared and inflated with a saline and contrast solution without any air contained, and the size is selected according to the proximal and distal reference vessel diameter. After advancing the IVL catheter to the target lesion guided by radiopaque markers on the catheter, the balloon is inflated at 4atm to contact with vessel wall, facilitating optimal energy delivery. By pushing a button on the cable connected the catheter, the lithotripsy cycle is activated and pulses once per second for ten seconds. After every cycle, the balloon is inflated up to 6 atm, which compresses the fractured calcium. The cycle is repeated as needed until the desired lesion expansion is obtained and the maximum repeatable cycle with the same catheter is 8 cycles.
Real-world Case Performed in Milan: Severely Calcified Lesion Treated With Shockwave IVL
Here is a representative case using this technology. A 73-year-old gentleman with past medical history of hypertension, dyslipidaemia and carotid artery atherosclerosis presented with typical stable anginal symptoms. Coronary angiography demonstrated severe stenosis in the left anterior descending (LAD) artery and left main coronary artery (LMCA) (Figure 1A-C). Following intubation with a XB 3.5 guiding catheter the lesion was wired with a BMW Universal coronary guidewire. The lesions were pre-dilated with a 1.5 and 2 mm non-compliant balloon, subsequent optical coherence tomography (OCT) revealed severe concentric calcification of LAD and LMCA (Figure 2A-C). In view of the severe calcification the lesions were further predilated with Shockwave 3 mm balloon in LAD and Shockwave 3.5 mm balloon in LMS (Figure 1A’-C’), according to vessel diameter on OCT. The shockwave IVL caused a crack the thick layer of calcium (Figure 2A’-C’). Subsequently, we implanted 3 overlapping drug eluting stents (DES) from LAD to LMCA (2.75 x 24 mm, 3 x 24 mm, 3.5 x 33 mm). Following DES implantation, we performed post-dilatation of the proximal stent and its overlap with 3.5 mm non-compliant balloon (28 atm). The residual distal LAD disease was treated with drug-coated balloon (2.5 x 30 mm). There was excellent final angiographic result (Figures 1a-c) and OCT (Figure 2a-c) images demonstrating well expanded and apposed DES.
Future Prospects For Intervascular Lithotripsy
The shockwave intravascular lithotripsy is an innovative approach for treating severely calcified lesions with PCI. Our initial clinical experience using IVL, for lesion preparation in real-world patients with severely calcified lesions, has been promising and resulted in excellent final angiographic and OCT results. Moreover, OCT imaging demonstrated that IVL was effective in cracking the thick (more than 180 degree) calcium burden.
IVL has the potential to be a permanent fixture in cardiac catheterization laboratories throughout the world, especially with an aging population who progressive exhibit higher prevalence of calcified lesions. A second generation device with improved crossing profile and deliverability is will be available in 2018. Furthermore, its ease of use (delivering a balloon to the lesion on any 0.014-inch guidewire), short learning curve and less procedural complications could facilitate rapid uptake. However, this is dependent on further studies demonstrating outcomes in patients, including comparisons with existing technologies.
Editor’s note: Editor’s note: Azeem Latib, M.D., is a senior interventional cardiologist at the Interventional Cardiology Unit, San Raffaele Hospital and EMO-GVM Centro Cuore Columbus, in Milan, Italy. His interests and experience are in complex coronary interventions, structural heart disease and new device innovation. He is also an Editorial Board member of DAIC magazine.
Latib also wrote the article “Transcatheter Annuloplasty For Repair Versus Replacement in Functional Mitral Regurgitation.”

 June 13, 2024
June 13, 2024