The Cardioband system is among several new transcatheter mitral repair systems entering clinical trials. In many cases, repair of the native valve is preferred over replacing the valve in open-chest surgical cases. This technology will allow a less invasive alternative.
The Cardioband System (Valtech) has recently been introduced as a potential option for transcatheter repair of the mitral valve among patients with functional mitral regurgitation (FMR). It has a CE mark in Europe, and a study to evaluate its safety and efficacy is planned in the United States.[1] Use of the Cardioband is intended to reduce the size of the annulus by placing an annuloplasty ring around it.
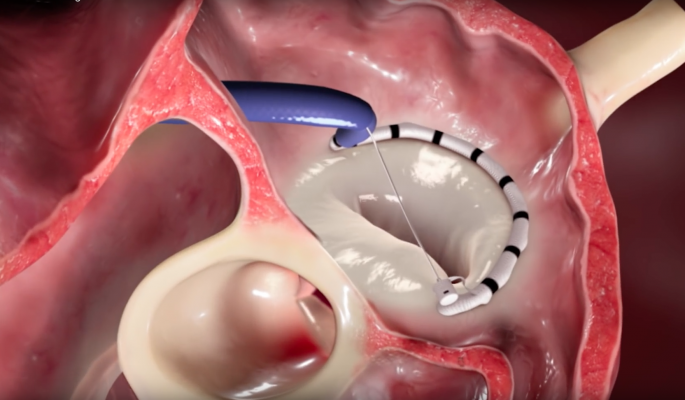
The left atrium is accessed through the fossa ovalis via the right atrium using a transvenous-transseptal approach. An annuloplasty band is implanted using transcatheter anchors. After implant deployment, a size adjustment tool is introduced over the wire to decrease the size of the annulus. As the procedure is performed in real time under beating heart conditions, and because the procedure is performed solely in the left atrium, it is associated with an excellent safety profile.
A 31-patient study in Europe demonstrated the feasibility of transcatheter annuloplasty for treatment of FMR, showing safety similar to other transcatheter mitral procedures and a high success rate of implantation with significant improvement in clinical outcomes.[2] Overall, 86.3 percent of patients achieved MR≤2+ at six-months and 55 percent MR≤1+. The investigators noted statistically significant improvement in six-minute walk test (6MWT), and in Minnesota Living with Heart Failure questionnaire (MLHFQ) and New York Heart Association (NYHA) classification at six months (P < 0.01 for both).
These data confirm my personal experience with the device. I believe Cardioband is a viable option for treatment of FMR, especially as it leaves future options available should the case merit additional intervention. In addition to confirming the safety and efficacy of this procedure, as well as a need to further refine patient selection, crucial questions remain regarding the learning curve associated with using the Cardioband and whether repair or replacement of the valve is preferable in FMR.
Watch the video “How to Implant the Transcatheter CardioBand Mitral Annuloplasty System.”
Assessing the Learning Curve
I first became involved in working with the Valtech Cardioband reconstruction system when my colleague at the time, Francesco Maisano, was performing the initial studies with the device, including the first procedure performed in human beings. My first impression of the Cardioband was that it is a potentially very difficult and challenging device to learn to use. However, after using the device myself over the past year, and after exposure to the company’s training program, I have learned that the steps of the procedure are reproducible and the learning curve is minimal. I have now performed nine procedures and feel comfortable with the techniques. I suspect that operators who have experience with other interventional mitral valve procedures, such as MitraClip, may find learning to use the Cardioband a little easier.
The MitraClip and Cardioband are obviously very different devices with different indications and different treatment objectives. Deciding on replacement versus reconstruction of the mitral valve in a patient with functional MR involves many factors, although fundamentally, there may be advantages to repair if it means future options are left viable. Considering the training elements of the two procedures, there are definite similarities in the navigation of the devices. However, the degree of control with the Cardioband in the left atrium is far superior, based on the fact that the operator is moving the device from anchor point to anchor point in a sequential fashion. The steps involved in Cardioband procedures are small and incremental compared with the need to navigate between the pulmonary artery and the mitral valve when using the MitraClip. It is my impression that the step-wise procedure of using a Cardioband is more reproducible, and, therefore, safer and easier to use.
Overall, I believe the Cardioband procedure is relatively straightforward to perform, especially if the operator has experience with mitral valve intervention, or at least some experience with transseptal puncture. One should also be familiar with transesophageal echo (TEE) and 3-D echocardiography and how to interpret them. As well, the operator should be fully versed in the mitral valve apparatus, which means it is a suitable procedure for interventional cardiologists and cardiac surgeons alike.
As I mentioned above, Valtech has created a training program for operators interested in learning about the Cardioband. Importantly, the company has developed a procedural protocol that is reproducible and that can be easily communicated to new operators. In addition, they have developed a simulator that recreates a very close facsimile of the human heart, complete with use of echocardiography and fluoroscopy during the mimicked procedure. I liken the Valtech program to learning to fly an airplane: the company has developed a flight manual and simulator that guide the new pilot through what he or she may encounter in about 95 percent of cases. Once versed in the fundamentals of the procedure, the operator has the confidence needed to adjust when unusual anatomy is encountered.
The hardest part of the procedure for me to adjust to was the use of imaging. Correct placement of the anchors depends on identifying anatomic landmarks and their relation to tissue of interest. The reliance on echocardiography for the procedure is a necessity, but it is also a limitation, as it takes skill to use the device properly and to interpret it correctly. Yet, the very nature of interventional procedures is that they spare the patient from the risks associated with open-heart procedures, and thus, there are inherent benefits to performing a procedure under beating heart conditions using imaging, as well.
As with most other procedures I have learned, I have become more comfortable with the techniques as I practiced them more — in both the simulator and in the cath lab. In the last two procedures I performed, I really started to feel comfortable with placing the anchors used to resize the annulus, as well as in interpreting the echocardiography images. That has led, in turn, to a significant decrease in procedure time.
A Different Context For Repair vs. Replacement
As more data on patients who are treated for functional MR using the Cardioband is gathered, I suspect we will learn more about the safety and effectiveness of this device. I think it will be significant for changing the treatment paradigm towards early intervention to repair the valve via annuloplasty before limiting options such as replacement are used. Ultimately, a decision between repair and replacement may factor on the patient’s anatomy, with repair being preferable unless the physiologic conditions dictate otherwise.
There are analogous lessons to be learned from the surgical management of functional MR with regard to repair versus replacement, where, as a general rule, repair is preferable. Similarly, it would stand to reason that interventional repair would be superior to replacement if the repair procedure is safe — while either interventional repair or replacement would be theoretically superior to surgery as a less invasive option. It may be misleading, however, to compare outcomes of repair versus replacement because one or the other may be more appropriate based on the underlying anatomy. Instead, it may be necessary to rethink how these approaches are used.
Most of the patients in whom I have used the Cardioband have low ejection fractions and a very dilated heart. These are patients who had advanced disease. It would be much more beneficial to intervene earlier in the disease course because there would be a better chance of achieving reverse remodeling. Instead of asking if it is better to repair or replace the valve, we should be asking if it is better to intervene early or late. It stands to reason that therapies that do not exclude future options are preferable, and it also makes sense that we should try to repair before we replace a dysfunctional valve.
Ultimately, what the Cardioband represents is an opportunity to rethink the debate over repair versus replacement. If the focus shifts to a question of early versus late intervention, then less invasive options become more preferable, and repair emerges as the better option. Interestingly, treatment of FMR already follows this paradigm to some extent, for medical therapy is considered the most appropriate initial therapy. Patients who fail to respond to medical approaches have their care elevated vertically, with open-heart surgery reserved for the most severe cases—and even when the chest is opened, repair is preferred over replacement. Thus, an interventional repair procedure, if proven safe and effective, offers the potential to actualize the overall treatment approach we already intuitively know to be the best course for our patients, wherein we attempt to be as minimally invasive while still yielding the best conditions for long-term success.
Edwards Lifesciences Corp. announced in December 2016 it agreed to acquire Valtech Cardio Ltd.
Editor’s note: Azeem Latib, M.D., is a senior interventional cardiologist at the Interventional Cardiology Unit, San Raffaele Hospital and EMO-GVM Centro Cuore Columbus, in Milan, Italy. His interests and experience are in complex coronary interventions, structural heart disease and new device innovation.
References:


 April 01, 2026
April 01, 2026 







