Figure 2: Angiography demonstrates a stenotic lesion in the mid right coronary artery, undilatable by standard high-pressure balloon angioplasty (inset, arrowheads). (B) Optical coherence tomography (OCT) cross-sectional (top) and longitudinal (bottom) images acquired before IVL and coregistered to the OCT lens (arrow in A) demonstrate severe near-circumferential calcification (double-headed arrow) in the area of the stenosis. (C) Angiography demonstrates improvement in the area of stenosis after IVL (inset; note the cavitation bubbles generated by IVL [black arrows]). (D) OCT cross-sectional (top) and longitudinal (bottom) images acquired post-IVL and coregistered to the OCT lens (white arrow in C) demonstrate multiple calcium fractures and large acute luminal gain. (E) Angiography demonstrates complete stent expansion with the semicompliant stent balloon (inset) without the need for high-pressure noncompliant balloon inflation. (F) OCT cross-sectional (top) and longitudinal (bottom) images acquired post-stenting and coregistered to the OCT lens (arrow in E) demonstrate further fracture displacement (arrow), with additional increase in the acute area gain (5.17 mm2), resulting in full stent expansion and minimal malapposition.
Over the last 40 years, despite multiple advancements in percutaneous coronary interventions, calcified lesions remain a challenge for even the most experienced operators leading to an increase in morbidity and mortality. Most recently, intravascular lithotripsy (IVL) has been shown to be an innovative technology that is designed to address heavily calcified lesions.
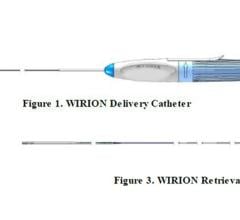
The Coronary Intravascular Lithotripsy Catheter (Shockwave Medical, Santa Clara, Calif.) is a single-use sterile disposable catheter that contains multiple lithotripsy emitters enclosed in an integrated balloon (Figure 1). The emitters create sonic pressure waves in the shape of a sphere, creating a field effect to treat circumferential vascular calcium. These sonic pressure waves selectively disrupt and fracture calcium in situ, altering vessel compliance, while minimizing injury and maintaining the integrity of the fibro-elastic components of the vessel wall. (Figure 2)
Details of the CAD I Study Leading to European Approval
Coronary IVL received European CE mark approval following the Disrupt CAD I Study,[1] which was initially presented at the 2016 Transcatheter Cardiovascular Therapeutics (TCT) conference. This study demonstrated a reduction in residual stenosis to 13.3±11.6% and acute luminal gain of 1.7±0.6 mm with low major adverse cardiovascular events (MACE) rates at 30 days and 6 months of 5% and 8.5% respectively.
The study investigators of CAD I concluded that coronary IVL was able to treat heavily calcified lesions with a low rate of complications and favorable initial treatment success. Disrupt CAD I included an optical coherence tomography (OCT) sub-study to determine the mechanistic effects of coronary IVL on heavily calcified coronary lesions with subsequent stent implantation.[2] Ziad Ali, M.D., associate director of Translational Medicine at the Center for Interventional Vascular Therapy, at Columbia University Medical Center/NewYork-Presbyterian Hospital, and the co-authors reported that OCT imaging identified calcium modification with fracture as a mechanism of action of coronary IVL. This modification allowed for significant acute area gain and favorable stent expansion in a difficult to treat anatomy.
Figure 2 highlights a case completed by Jonathan Hill, M.D., is a consultant cardiologist at King’s College Hospital in London, during the CAD I Study. Coronary angiography demonstrates expansion both after IVL and the stent placement, while OCT images show multiple calcium fractures that increase in size after stent placement and full stent expansion.
Additional clinical experience is being conducted in Europe under the Disrupt CAD II Study. CAD II will enroll an additional 120 patients at 15 sites across eight European countries with the goal of presenting outcomes in a real-world, post-market setting.
Disrupt CAD III U.S. FDA Pivotal Trial
The first enrollment in the pre-market Disrupt CAD III U.S. investigational device exemption (IDE) Study was recently announced. Disrupt CAD III is a prospective, non-randomized, multicenter global IDE study to demonstrate the safety and effectiveness of the Shockwave Coronary IVL System with the Shockwave C2 Coronary IVL Catheter in de novo, calcified, stenotic, coronary arteries prior to stenting. Patients with de novo, calcified coronary artery lesions presenting with stable, unstable or silent ischemia that are suitable for percutaneous coronary intervention (PCI) will be considered for study participation. The study is expected to enroll approximately 392 patients at 50 global centers in the United States and Europe. The Shockwave C2 Coronary IVL Catheter is an investigational device in the U.S.
The study will assess freedom from MACE within 30 days of the index procedure as the primary safety endpoint. The primary effectiveness endpoint is procedural success which, based on predicate studies, is defined as stent delivery with a residual stenosis of less than 50 percent and without in-hospital MACE. Enrolled study patients will be followed for two years.
Richard Shlofmitz, M.D., chairman, Department of Cardiology, St. Francis Hospital in Roslyn, N.Y., enrolled the first patient. The coronary IVL technology being investigated in the United States and Europe has been highly anticipated. This pivotal, core-lab adjudicated study will add to the available clinical evidence and be submitted to FDA for a pre-market application.
Atherectomy and High-pressure Balloons vs. Lithotripsy to Treat Calcified Lesions
Current techniques to treat calcified, coronary lesions include rotational and orbital atherectomy. However, the adoption has been limited. Atherectomy preferentially targets superficial calcium without significant impact to medial calcium. High pressure and specialty balloons are also available, but often fail to reach or cross the calcified lesion and similar to atherectomy, only address superficial calcification. Neither atherectomy nor balloons differentiate calcific plaque from soft tissue, which can lead to vessel trauma and potential complications.
In reviewing both the Disrupt CAD I outcomes and the real-world utilization in Europe, Australia and New Zealand, IVL appears to have benefits over current technology. It is the only technology that impacts both superficial and deep calcification, which provides improved transmural vessel compliance. This allows for better stent deployment, expansion and apposition. It utilizes a balloon-based system that all operators are familiar with, which facilitates easy adoption and reduces learning curve compared to other, more complex, technologies. It can also be used in technically challenging lesions, such as bifurcation or ostial lesions, without concerns of wire bias, perforation or increased risk of embolization. Indeed, from both the patient and physician perspective, the apparent lack of athero-embolization, perforation or need for high-pressure balloon dilatation (barotrauma) with the attendant risk of vessel dissection, are all very attractive attributes of IVL.
Intravascular Lithotripsy To Enable Passage of Large-bore Devices
In addition to the coronary technology, a growing number of interventionalists are adopting the use of IVL to facilitate trans-femoral access in procedures that require large bore catheter delivery systems, such as trans-aortic valve replacements (TAVR) and mechanical cardiac support. In these cases, IVL fractures calcium, increasing the luminal diameter and improving compliance, which allows the device to safely pass through the iliac artery and ultimately be delivered/placed in the heart.
Carlo Di Mario, M.D., Ph.D., Imperial College London, and colleagues recently published a case series of 42 patients in which IVL enabled TF access in patients undergoing TAVR that would have otherwise required alternative access, preserving the well-known benefits of TF access.[3] In addition to iliac preparation pre-TAVR, IVL can also facilitate Impella access for mechanical cardiac support of high risk PCI or cardiogenic shock. A recent case report demonstrated the feasibility of such an approach and a broader case series looking at the safety and effectiveness of this is currently being prepared for submission.[4]
Editor’s note: The authors of this article are doctors Dean Kereiakes and Jonathan Hill, the co-principal investigators of the DISRUPT CAD III clinical trial. Dean Kereiakes, M.D., FACC, FSCAI, is medical director of The Christ Hospital Heart and Vascular Center in Cincinnati, Ohio. Jonathan Hill, M.D., is a consultant cardiologist at King’s College Hospital in London.
Related Lithoplasty Content:
VIDEO: How a Lithoplasty Balloon Shatters Calcified Plaque in Arteries With Ultrasound
Shockwave Announces Collaboration With Abiomed on Physician Training
Shockwave Initiates U.S. Pivotal Study for Coronary Intravascular Lithotripsy
Lithotripsy Safe and Effective in Calcified Stenotic Peripheral Arteries
Intravascular Lithotripsy May Offer Solution for Calcified Coronary Lesions
Shockwave Launches Coronary Intravascular Lithotripsy in Europe
First U.S. Patient Treated in DISRUPT PAD III Study of Lithoplasty Technology
References:
1. Brinton, T.J., Ali, Z., Hill, J., Meredith, I., Maehara, A., Lanksy, A., Gotberg, M., Van Mieghem, N., Whitbourn, R., Fajadet, J., Di Mario, C., Feasibility of Shockwave Coronary Intravascular Lithotripsy for the Treatment of Calcified Coronary Stenoses: First Description. Circulation, 2019;139:834–836.
2. Ali ZA, Brinton TJ, Hill JM, Maehara A, Matsumura M, Karimi Galougahi K, Illindala U, Gotberg M, Whitbourn R, Van Mieghem N, Meredith IT, Di Mario C and Fajadet J. Optical Coherence Tomography Characterization of Coronary Lithoplasty for Treatment of Calcified Lesions: First Description. JACC Cardiovasc Imaging. 2017;10:897-906.
3. Carlo Di Mario, M.G., Francesca Ristalli, Marcello Ravani, Francesco Meucci, Miroslava Stolcova, Gennaro Sardella, Nicolo Salvi, Francesco Bedogni, Sergio Berti, Vasilis Babaliaros, Andrei Pop, David Caparrelli, James Stewart, Chandan Devireddy, A Prospective Registry of Intravascular Lithotripsy Enabled Vascular Access for Transfemoral Transcatheter Aortic Valve Replacement JACC: Cardiovascular Interventions. 2019; 12(5): 502-504.
4. Riley, R, Corl, J, Kereiakes, D. Intravascular lithotripsy-assisted Impella insertion: A case report. Cather Cardiovasc Inter. 2019; 1-3. DOI: 10.1002/ccd.28168.


 November 08, 2024
November 08, 2024