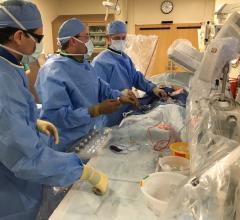
Some of the device technologies discussed in the TCT 2020 late-breaking trial sessions. Top left, the Medtronic Resolute Onyx stent was the first stent to receive FDA clearance for short duration dual-antiplatelet therapy, which was a big topic and subject of several sessions. Lower left, the Keystone TriGuard 3 TAVR embolic protection device did not demonstrate superiority over TAVR without use of embolic protection. Top right, the Abbott MitraClip was the subject of two studies, including use to aid heart transplant patients. Bottom right, the Boston Scientific Acurate neo TAVR valve performed below the Sapien 3 and CoreValve Evolut.
Here are some of the key takeaways from the late-breaking interventional cardiology and structural heart trials presented at the 2020 Transcatheter Cardiovascular Therapeutics (TCT) meeting in October.
1. Shortened DAPT for Drug-eluting Stents
The use of short duration dual-antiplatelet therapy (DAPT) has been a big topic of discussion at TCT the past few years. The first U.S. Food and Drug Administration (FDA) cleared indication for shortened DAPT was granted in late September 2020 for the Medtronic Resolute Onyx stent. The data from two late-breaking trials at TCT will likely lead to the Abbott Xience receiving a similar FDA indication expansion.
Medtronic's FDA indication is for one month of DAPT for high bleeding risk (HBR) patients implanted with the Resolute Onyx Drug Eluting Stent (DES). It was the first DES in the U.S. that has been proven safe and effective utilizing a one-month regimen of DAPT following a percutaneous coronary intervention (PCI) in patients at high bleeding risk. Patients that are at risk for high bleeding include older patients, those with history of bleeding, or those on oral blood-thinning drugs, and account for up to 40 percent of PCI patients. Clinical studies demonstrated that Resolute Onyx DES and its biocompatible polymer and stent design promoted fast vessel healing and is well-suited for patients who may benefit from a DAPT duration as short as one month.
Shortened DAPT was the subject of several late-breaking studies at TCT 2020.
Results from the XIENCE 90/28 trials reported at TCT 2020 showed the safety of shortening DAPT with the Abbott Xience stent to 28 and 90 days, rather than the standard of one year. The trial adds more validity to shortening DAPT in patients who are at higher risk for bleeding.
“Among high bleeding risk patients undergoing PCI with the Xience stent, a short DAPT regimen of one or three months compared with standard DAPT up to 12 months resulted in non-inferior ischemic outcomes and similar rates of clinically relevant (BARC 2-5) bleeding, with a significant reduction in major (BARC 3-5) bleeding. Additionally, there was a very low incidence of stent thrombosis.” said Roxana Mehran, M.D., director of interventional cardiovascular research and clinical trials, The Zena and Michael A. Wiener Cardiovascular Institute at Mount Sinai.
The Boston Scientific Synergy DES also showed good results with shortened DAPT in the late-breaking EVOLVE Short DAPT study presented at TCT 2019. Watch the VIDEO: Early Discontinuation of DAPT in High Bleeding Risk Patients With the Synergy Stent — interview with Ajay J. Kirtane, M.D.
The results for the Medtronic and Abbott devices did not translate to other technologies designed specifically to help shorten DAPT. The COBRA-REDUCE trial results were presented at a late-breaking trial at TCT, and the use of the nanotechnology polymer-coated Cobra PzF stent plus 14-day DAPT did not reduce bleeding or establish non-inferior outcomes for thrombotic events compared with the Xience, Promus or Resolute DES and standard three- or six-month DAPT therapy.
The COBRA-REDUCE trial was a randomized, open-label, active-controlled, assessor-blinded, multi-center trial. A total of 996 patients were enrolled between February 2016 and May 2020 at 59 sites in Europe and the United States. Patients at high bleeding risk (HBR) due to requirement for oral anticoagulation were randomized at the time of PCI to treatment with the COBRA-PzF stent followed by a very short duration (14 days) of DAPT or an FDA-approved new generation DES followed by guideline-recommended DAPT duration (three or six months).
Read more in the article Nano-Coated Coronary Stent and Shorter DAPT Did Not Meet Non-inferiority for Thrombotic Events.
VIDEO: Use of Shorten DAPT and the Xience Stent in High-bleeding Risk Patients — Press conference presented by Roxana Mehran, M.D., and Marco Valgimiggle, M.D.
Shorter DAPT With Xience Stent is Noninferior to Standard DAPT
2. Intravascular Lithotripsy Safely Treats Severely Calcified Coronary Lesions
The positive results from the late-breaking Disrupt CAD III study presented at TCT will likely pave the way for FDA clearance for intravascular lithotripsy in the coronary arteries. The study showed the Shockwave Medical Intravascular Lithotripsy system was safe and effective in breaking up these difficult to treat lesions and had much less vessel trauma compared to the current techniques of atherectomy, cutting balloons and high pressure balloons. The technology uses a compliant balloon and uses sonic waves to bust the calcium rather than breaking using brute force. This could be a paradigm shift in how calcified lesions are treated in the future, said Dean Kereiakes, M.D., medical director, The Christ Hospital Heart and Vascular Center, medical director, The Christ Hospital Research Institute, and professor of clinical medicine at The Ohio State University, who presented the data.
VIDEO: Intravascular Lithotripsy to Treat Severely Calcified Coronary Artery Lesions
VIDEO: Demonstration of Intravascular Lithotripsy Breaking Up Calcium
3. No Mortality Risk Found With Paclitaxel-coated Devices
A meta-analyses published in December 2018 of randomized trials of paclitaxel drug-coated devices (DCD) reported increased long-term mortality compared with non-DCD in the treatment of peripheral artery disease (PAD). This prompted an FDA warning about the use of DCD in patients with PAD. It also spurred a huge amount of debate in the interventional community about the safety of paclitaxel. At TCT 2019, one day of the FDA town hall meeting was devoted to this topic and the key takeaway was that more data was needed to show either safety of DCDs or to clarify what is causing any increased mortality issues.
The late-breaking VOYAGER PAD Trial at TCT 2020 is the first large scale study to examine this and confirm the safety of paclitaxel devices. The large, randomized, subgroup analysis of 6,564 patients showed neither a mortality risk nor benefit associated with the use of paclitaxel DCD. The study also found that the benefit of rivaroxaban use on reducing ischemic limb and cardiovascular outcomes was consistent regardless of whether a DCD was used.
Read more details in the article No Mortality Risk Associated With Paclitaxel-coated Devices Used to Treat Peripheral Artery Disease.
4. Durable Polymer Stents May be Better Than Bioresorbable Polymer DES
In a surprise to many, the randomized HOST-REDUCE-POLYTECH-ACS clinical trial found DES that used a durable polymer are non-inferior to DES with biodegradable polymers in patients with acute coronary syndrome (ACS). The 3,400-patient study is the first large-randomized study to compare durable polymer to biodegradable polymer stents, and the findings surprised many experts who thought bioresorbable polymers would easily out-perform the older generation durable polymer stent technology.
Durable polymers have been implicated in the Achilles heel of DES, which is late-stent thrombosis that can occurs years after a stent implant due to the polymers causing a chronic inflammatory response within the vessel wall. Bioresorbable polymers dissolve after a couple years and were supposed to solve this problem and prevent late events.
In the primary outcome measure, biodegradeable polymer stents had a higher rate of significant stenosis in the short term at one year compared to durable polymer stents, 6.4 vs. 5.2 percent. Secondary outcome measures for cardiac death, target vessel myocardial infarction and target lesion revascularization (TLR) were also in favor of durable polymers (3.9 vs. 2.6 percent). TLR rates alone were 1.8 vs. 1 percent in favor of durable polymer stents.
"There was a sign of high numbers of clinical events in the biodegradable, rather than the durable polymer DES. The message is that the hypothesis that biodegradable stents would be better is not actually correct," explained Ori Ben-Yehuda, M.D., executive director of the CRF Clinical Trials Center.
"I was a little surprised by these results," explained Robert Yeh, M.D., director of the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology at the Beth Israel Deaconess Medical Center, and associate professor of medicine at Harvard Medical School. He was on the expert panel at the press conference presentation. He is suspicious of the early separation between the groups with cardiac events and wonders if this early separation is due to peri-procedural issues rather than with the stents. Yeh said earlier trials showed the Orsiro stent outperformed the Xience, so it is very surprising to see a group of stents with Orsiro not perform at least as well as Xience and like stents in this study, he said.
"My main takeaway from this study is that if it is not showing a harm signal for biodegradable polymer DES, it certainly is not showing a benefit, so the question is what is the place for this line of technologies if at the very least we can't demonstrate a substantial benefit over a durable polymer stents," Yeh said.
Read more in the article Durable Polymer Drug-Eluting Stents Perform Better Than Biodegradable Polymer DES.
5. TAVR Cerebral Embolic Protection Trial Shows Little Difference in Stoke Rates
The stroke rates were initially high in transcatheter aortic valve replacement (TAVR) compared to surgical aortic valve replacement (SAVR) trials, but these rates have decreased in recent years as TAVR operators become more proficient during the procedures and the stroke rates are now comparable or lower than SAVR. Cerebral embolic protection devices were developed to prevent emboli knocked off the aortic walls and from the aortic valve from traveling to the brain in an effort to lower the higher stroke rates from a few years ago. A late-breaking study from the STS/ACC Transcatheter Valve Registry (TVT) presented at TCT showed the impact of using cerebral embolic protection devices appears to be minimal.
This review of embolic protection device performance and use showed 66 percent of the 700 sites in the TVT Registry report not using these devices. The rate of in-hospital stroke in the embolic protection group of patients was 1.39 percent. The rate of stroke in patients without embolic protection was 1.54 percent. There was no difference inn the rates of death, stroke, major bleeding or device success between these two groups, said David Cohen, M.D., chair in cardiovascular clinical research at Saint Luke’s Mid America Heart Institute in Kansas City, who presented the study.
The study also included a propensity-weighted analysis where the embolic group has a stroke rate of 1.3 percent and the no protection device group at 1.58 percent.
Cohen said there was not a significant reduction in in-hospital or 30-day stroke rates. While there its a slight signal toward fewer strokes with embolic protection, he said the findings show clinical equipoise and provide strong rational for ongoing, large-scale randomized, controlled trials to see if embolic protection devices offer meaningful clinical benefit.
This data was reinforced by another late-breaker, the REFLECT II randomized clinical trial evaluating the safety and efficacy of the Keystone Heart TriGuard 3 (TG3). The self-stabilizing cerebral embolic deflection filter used in patients undergoing TAVR met the primary safety endpoint, but did not demonstrate superiority over TAVR without use of embolic protection.
“Compared to controls, the primary 30-day safety endpoint was higher with TriGuard 3 due primarily to TAVR related vascular and bleeding complications,” said Jeffrey W. Moses, M.D., professor of cardiology at Columbia University Vagelos College of Physicians and Surgeons, director of interventional cardiovascular therapeutics, NewYork-Presbyterian/Columbia University. “While the study did not demonstrate superiority of TriGuard 3 compared to pooled controls for the primary hierarchical efficacy endpoint, a post hoc DW-MRI analysis suggests that TG3 may reduce larger ischemic lesions. Improved device stability to achieve reliable, complete cerebral coverage may improve outcomes.”
Read more in the article Keystone Heart TAVR Embolic Protection Device Did Not Demonstrate Superiority.
6. Acurate Neo TAVR Valve Does Not Measure Up to Sapien or Corevalve
Boston Scientific's self-expanding TAVR valve Acurate neo failed to show non-inferiority to the Medtronic CoreValve or Edwards Lifesciences Sapien 3 valves.
The SCOPE II trial comparing the Acurate neo vs. CoreValve Evolut failed to demonstrate non-inferiority. This was the same negative result as the SCOPE I trial presented at TCT 2019, where a comparison with the Acurate Neo vs. Sapien also did not meet non-inferiority.
Death or stroke at one year was 15.8% in the Acurate neo group compared to 13.9% in the CoreValve Evolut group. The rate of moderate-severe aortic regurgitation was 9.6% vs 2.9% at 30 days and 4 % vs. 3.3% at one year.
New pacemaker implantation at 30 days was 10.5% with Acurate neo compared to 18% with CoreValve Evolut. Cardiac death at 30 days was 2.8 vs. 0.8%, and one year was 8.4 vs. 3.9%, was greater in the Acurate neo group.
Read more details in the article Acurate neo TAVR Valve Fails to Meet Noninferiority With Medtronic CoreValve Evolut.
Longer-term follow-up from the SCOPE I trial presented at TCT 2020 showed the Acurate neo had similar outcomes and functional improvements compared the the Sapien 3, but the 30-day rate of paravalvular regurgitation remained significantly higher with Acurate neo.
Boston Scientific last fall said it hoped to overcome the shortcomings of the first generation device with the improved design in the new Acruate Neo2 valve. That valve just gained European CE mark approval in September 2020. Experts on the panel discussing the trials said it will become more difficult for new transcatheter valves to match or out perform the Sapien 3 or CoreValve because these devices now have so much clinical experience and have undergone numerous iterations to improve these devices.
7. No Advantage to Transcatheter Closure of ASDs caused by MitraClip Implants
The MITHRAS randomized clinical trial found that interventional closure of an iatrogenic atrial septal defect (iASD) required to perform transcatheter mitral valve repair (TMVR) was not superior to conservative medical treatment when measured in the patients performance in a six minute walk test. TMVR requires transseptal access to the left atrium, which creates an iASD that remains with detectable shunting across the intra-atrial septum. While the induction of an iASD has been linked to improved hemodynamics in specific heart failure populations and is currently being investigated in large-scale clinical trials in patients with heart failure, the presence of a persistent iASD is also associated with increased long-term mortality and morbidity following TMVR.
The prospective, randomized, single-center trial had 80 patients with a persistent iASD one month following TMVR and relevant left-to-right shunting were randomly assigned in a 1:1 ratio to standard medical therapy alone or closure of the iASD using the Occlutech ASD occluder. The primary endpoint was change in 6-minute walk distance five months after iASD occlusion. Secondary endpoints included all-cause mortality and rate of heart failure hospitalization at one year.
“Interventional closure of iASD one-month post transcatheter mitral valve repair was not superior to conservative treatment with regard to the primary endpoint six-minute walking distance,” said Philipp Lurz, M.D., Ph.D., Deputy Head of the Cardiology Department at Heart Center Leipzig at the University of Leipzig, Germany. “The results are corroborated by no difference in secondary endpoints such as heart failure symptoms or hospitalization and survival. The presence of an iASD is associated with a higher rate of HF hospitalization irrespective of its management when compared to patients without relevant iASD following TMVR. The presence of an iASD following transcatheter mitral valve interventions might be a prognostically relevant surrogate, but not necessarily causative for inferior outcomes.”
Read more in the article Transcatheter Closure of Residual ASD After Transcatheter Mitral Valve Repair Was Not Superior to Medical Therapy.
8. Local vs. General Anesthesia for TAVR
The use of general vs. local anesthesia in TAVR was examined by the late-breaking SOLVE-TAVI one-year outcomes trial. It showed both approaches are safe to use and the outcomes are good, so it can be a matter of preference.
TAVR centers have been moving toward the procedure becoming a same day surgery to reduce overnight admissions and send them home as an outpatient procedure. This can be accomplished using a local anesthesia if transesophageal echo (TEE) is not needed. However, many centers still use TEE for procedural guidance. Local anesthesia generally has a faster recovery time and reduces potential complications in sicker and older patients.
VIDEO: General vs Local Anesthesia for TAVR Addressed in SOLVE-TAVI Trial
9. MitraClip As a Bridge to Heart Transplant
The MitraBridge Study showed the transcatheter MitraClip mitral leaflet repair system can be used as bridge therapy for patients on the heart transplant list. It was used to reduce the amount of mitral regurgitation to help ease symptoms in advanced heart failure who need a need a heart transplant, but may have to wait long periods before a heart becomes available.
The 119-patient study found it not only helped improve patient symptoms for the majority of patients, but 23.5 percent of patients in this study improved so much they were actually taken off the transplant.
There is a large and growing imbalance between the demand and supply of donor hearts, explained study presenter Cosmo Godino, M.D., an interventional cardiologist from San Raffaele Hospital, Milan, Italy. With the expansion of waiting lists and prolonged waiting times are generally more than a year and it becomes difficult to manage these patients, resulting in a one-year mortality rate of 15 percent.
Patients selected for MitraClip had advanced/end stage heart failure and concomitant, severe mitral regurgitation with a median left ventricular ejection fraction of 26%. These patients make up between 1 to 10% of the overall heart failure population, Godino said.
There was an 87.5% procedural success rate and no deaths at 30-day. Two thirds of patients remained free of development of composite adverse events at one-year. Of those that improved, 15.5% become eligible for a heart transplant. nearly a quarter could be removed from the list for HTx due to clinical improvement
Watch the press conference presentation of the data in the VIDEO: Use of MitraClip as a Bridge to Heart Transplant.
10. Pre-emptive Treatment of Vulnerable Plaques Using Bioresorbable Stents
The PROSPECT ABSORB Trial was started prior to the Abbott Absorb fully bioresorbable stent being pulled off the market because of performance below that of metallic stents. However, it was tested in this provocative study to preemptively stent high-risk vulnerable plaques with a bioresorbable scaffold before the lesions rupture and cause a heart attack. Patients were randomized to PCI using an Absorb bioresorbable vascular scaffold (BVS) stents vs. guideline directed medical therapy (GDMT).
This is the first study that proactively identified and preemptively treated vulnerable plaques.
Lesion-related major adverse cardiac events (MACE) events at four years showed medical therapy alone resulted in 10.7 percent events and the BVS treat patients were 4.3 percent. Study Principal Investigator Gregg Stone, M.D., said the favorable BVS MACE rates warrants a larger, adequately powered randomized trial to determine if PCI treatment of focal vulnerable plaques improves patient outcomes over the long term, rather than using PCI in a reactive fashion after a patient has had a heart attack and might have suffered permanent damage to the heart.
Watch the press conference presentation of the data in the VIDEO: Pre-emptive Treatment of Vulnerable Plaques With Bioresorbable Stents.
Links to all the TCT 2020 Late-breaking Study Presentations
 August 28, 2023
August 28, 2023